
12 Studies Later: Robust Evidence in Curing Insomnia

Main Points
Cognitive behavioral therapy showed consistent benefits for insomnia across 12 studies. In one trial of people diagnosed with chronic insomnia disorder, more than 70% of those receiving CBT reached the threshold for normal sleep efficiency, and almost 40% reached 90% sleep efficiency.
In-person CBT may be more effective than online CBT, although both approaches improved insomnia severity. Follow-up data suggest that the benefits can be maintained for months after treatment.
CBT for insomnia combines stimulus control, sleep monitoring, sleep hygiene, education, bedtime routines, and sleep restriction. It can be done at home, but it requires consistency and effort. When possible, working with a professional appears to be the strongest option.
Insomnia can affect far more than sleep. When a person struggles to fall asleep, stay asleep, or feel restored by sleep, the effects can spill into daily energy, mood, focus, and overall quality of life. Instead of focusing on another sleep supplement, the evidence reviewed here centers on cognitive behavioral therapy, or CBT, as a practical approach for improving insomnia.
Across 12 studies [826-837], CBT consistently showed benefits for sleep. One trial [826] helps illustrate how effective it can be. In that study, 164 people diagnosed with chronic insomnia disorder were divided into three groups: one received CBT (cognitive behavioral therapy), another received imagery relief therapy, and the final group continued with usual prescriptions and counseling from their doctor. A key outcome was sleep efficiency.
Sleep efficiency is a combined measure of several key aspects of sleep quality. It includes sleep onset latency, which refers to the amount of time it takes a person to fall asleep. It also accounts for wake after sleep onset, or the amount of time a person spends awake after initially falling asleep. Finally, it considers the total time spent in bed, whether the person is asleep or awake.
Sleep Efficiency and Insomnia Resolution
A sleep efficiency score of 80% or higher is considered normal sleep. When the trial measured how many people reached different levels of sleep efficiency, the results were striking.
More than 70% of people who received CBT reached at least 80% sleep efficiency, meaning their insomnia was considered resolved by that definition. Almost 40% reached 90% sleep efficiency, which reflects excellent sleep efficiency.
These were not people with mild sleep complaints. They had been diagnosed with insomnia disorder, so the improvements represented meaningful changes.
The follow-up data were also important. Two months after CBT ended, some decline appeared compared with the immediate post-treatment results, but a significant amount of improvement remained, especially in the group reaching 80% sleep efficiency.
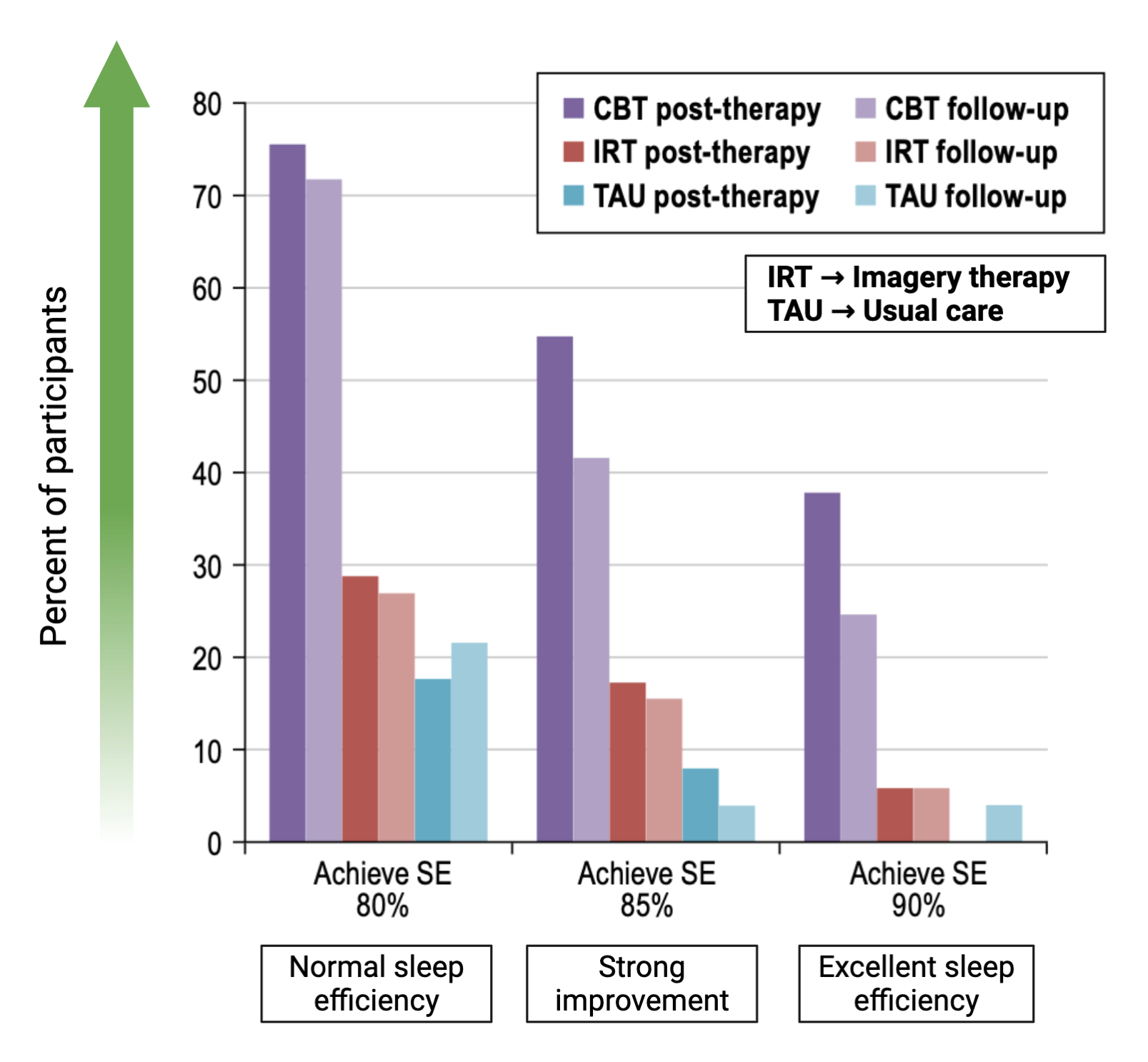
The other treatment groups showed little change, suggesting that CBT was uniquely effective for many people with insomnia.
There are limitations. In this trial, participants tracked their sleep using sleep diaries rather than sleep trackers or other objective tools. Scientifically, that is a weakness. At the same time, it also gives a real-world view of how people with insomnia perceived their own sleep. They reported meaningful improvements in a problem that directly affects daily life.
Other studies [834] using more objective measures also showed similar benefits from CBT.
Online CBT Versus In-Person CBT
One important difference across the studies is how CBT was delivered. Some trials used online CBT, while others used in-person CBT.
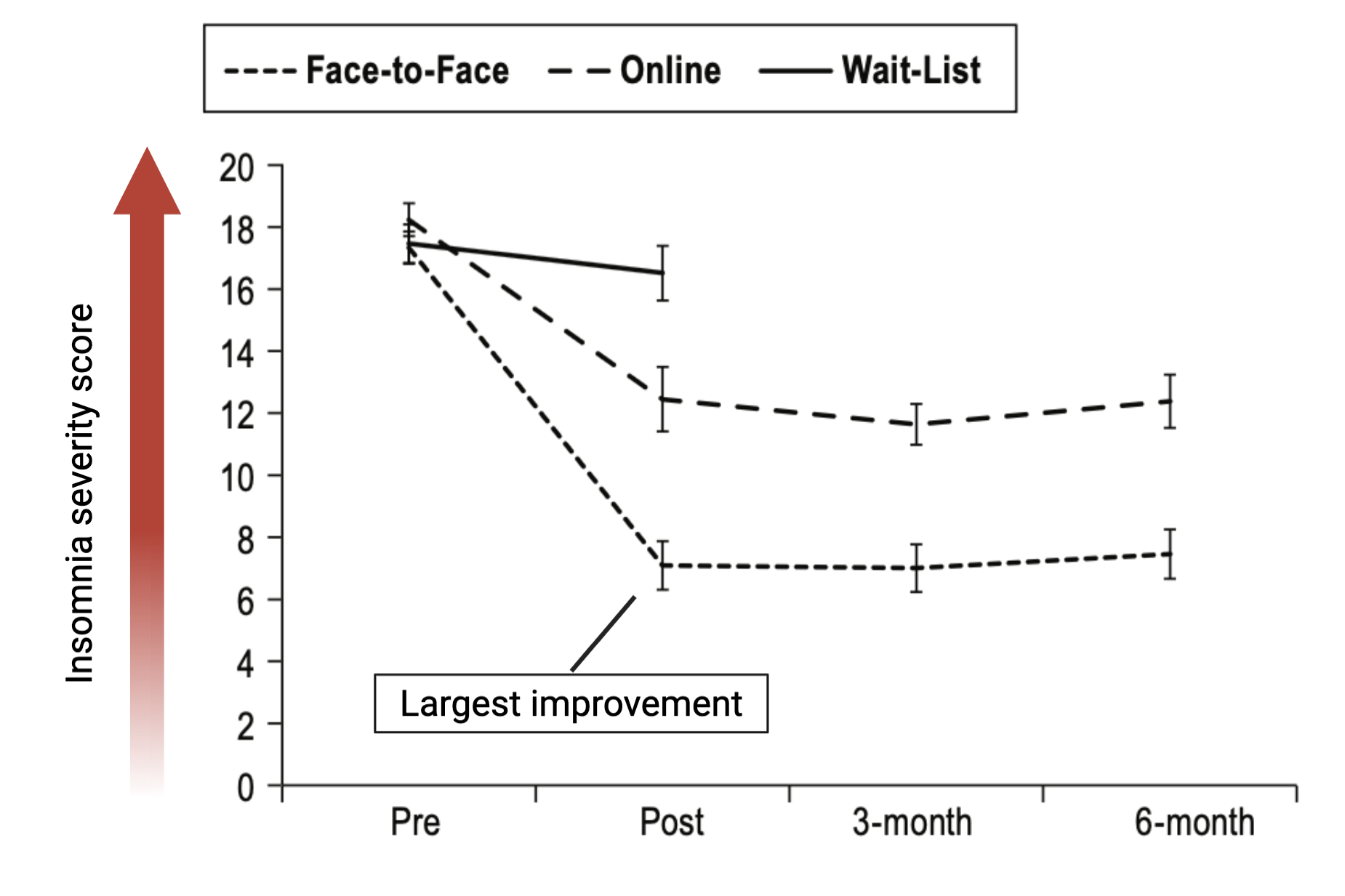
Evidence suggests that in-person CBT may be more effective than online CBT. In one study [828] comparing guided online CBT, face-to-face CBT, and a wait-list control group, both CBT approaches improved insomnia severity. The wait-list group showed little change, while both CBT groups improved. However, the face-to-face CBT group showed a larger reduction in insomnia severity.
Based on that study, the preferred approach would be to work with a professional in person when possible. Still, online or at-home CBT can also produce meaningful improvements.
The follow-up data from that same study add to the strength of the finding. At three and six months, insomnia severity remained much lower than where it started. That suggests the sleep improvements were not just short-term effects, but were maintained over time.
Specific Sleep Areas of Improvement by CBT
CBT on Depression, Anxiety, and Pain
CBT Protocol based on 10+ Studies
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
What CBT for Insomnia Includes
CBT is not one single technique. It is a combination of strategies, some intuitive and others more counterintuitive.
The more intuitive parts include stimulus control, limiting caffeine and alcohol, and avoiding overstimulation of the mind before sleep. CBT also includes more structured practices such as sleep monitoring, keeping a sleep diary, improving sleep hygiene, learning about sleep, creating a proper sleep environment, and building consistent bedtime routines.
One of the more counterintuitive parts is sleep restriction. In the early phases, CBT may intentionally restrict sleep to build stronger sleep pressure and help restore a more predictable sleep pattern. Sleep is regulated by circadian rhythm and the sleep-wake process, including the buildup of adenosine. By temporarily restricting sleep and then gradually reintroducing it, CBT aims to help the body return to a more consistent rhythm.
If you are interested in trying this yourself, though preferably with a professional guiding you, here is a free CBT course. There are also additional resources supplied by Stanford University, here. In addition, the US Department of Veteran Affairs has developed a free, no commercial interest, app for your phone called CBT-i Coach.
Main Points
Cognitive behavioral therapy showed consistent benefits for insomnia across 12 studies. In one trial of people diagnosed with chronic insomnia disorder, more than 70% of those receiving CBT reached the threshold for normal sleep efficiency, and almost 40% reached 90% sleep efficiency.
In-person CBT may be more effective than online CBT, although both approaches improved insomnia severity. Follow-up data suggest that the benefits can be maintained for months after treatment.
CBT for insomnia combines stimulus control, sleep monitoring, sleep hygiene, education, bedtime routines, and sleep restriction. It can be done at home, but it requires consistency and effort. When possible, working with a professional appears to be the strongest option.
References
[Study 826] Espie CA, Kyle SD, Williams C, Ong JC, Douglas NJ, Hames P, Brown JSL. A randomized, placebo-controlled trial of online cognitive behavioral therapy for chronic insomnia disorder delivered via an automated media-rich web application. Sleep. 2012;35(6):769-781. doi:10.5665/sleep.1872
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, the article stated that this was not an industry-supported study, but the software and web development were supported by Sleepio Limited; Dr. Espie was Clinical and Scientific Director of Sleepio Limited and a shareholder, Dr. Hames was Managing Director/CEO of Sleepio Limited and received a salary from the company, Dr. Williams was Director of Five Areas Limited, and the other authors reported no financial conflicts of interest.
[Study 827] van Straten A, Emmelkamp J, de Wit J, Lancee J, Andersson G, van Someren EJW, Cuijpers P. Guided Internet-delivered cognitive behavioural treatment for insomnia: a randomized trial. Psychol Med. 2014;44(7):1521-1532. doi:10.1017/S0033291713002249
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, financial support was received from Fund NutsOhra grant 0804–46 to develop the intervention and carry out the study; Industry Funding: From the study, no industry funding source was reported, and the declaration of interest stated none.
[Study 828] Lancee J, van Straten A, Morina N, Kaldo V, Kamphuis JH. Guided online or face-to-face cognitive behavioral treatment for insomnia: a randomized wait-list controlled trial. Sleep. 2016;39(1):183-191. doi:10.5665/sleep.5344
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, the online and face-to-face treatments were made possible by financial support from VGZ insurance company, and the authors indicated no financial conflicts of interest.
[Study 829] Horsch CHG, Lancee J, Griffioen-Both F, Spruit S, Fitrianie S, Neerincx MA, Beun RJ, Brinkman WP. Mobile phone-delivered cognitive behavioral therapy for insomnia: a randomized waitlist controlled trial. Journal of Medical Internet Research. 2017;19(4):e70. doi:10.2196/jmir.6524
Funding/Conflicts: Public Funding: From the study, funding was provided by Technology Foundation STW and the Nationaal Initiatief Hersenen en Cognitie under the Healthy Lifestyle Solutions partnership program; Non-Profit Funding: From the study, no separate non-profit funding source was reported; Industry Funding: From the study, funding was provided by Philips, and the authors declared no conflicts of interest.
[Study 830] Zachariae R, Amidi A, Damholdt MF, Clausen CDR, Dahlgaard J, Lord H, Thorndike FP, Ritterband LM. Internet-delivered cognitive-behavioral therapy for insomnia in breast cancer survivors: a randomized controlled trial. Journal of the National Cancer Institute. 2018;110(8):880-887. doi:10.1093/jnci/djx293
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, the work was funded by TrygFonden grant No. 7-12.0736 and the Danish Cancer Society grant No. R48-A2585-11-S3, and the funders had no role in the study design, data collection, data analysis, data interpretation, or writing of the report; Industry Funding: From the study, no industry funding source was reported, but Drs. Ritterband and Thorndike had equity ownership in BeHealth Solutions, LLC, which licensed the SHUTi program and software platform from the University of Virginia; the company had no role in preparing the manuscript, and the remaining authors declared no conflicts of interest.
[Study 831] Van der Zweerde T, Lancee J, Slottje P, Bosmans JE, Van Someren EJW, van Straten A. Nurse-guided internet-delivered cognitive behavioral therapy for insomnia in general practice: results from a pragmatic randomized clinical trial. Psychotherapy and Psychosomatics. 2020;89(3):174-184. doi:10.1159/000505600
Funding/Conflicts: Public Funding: From the study, the trial was funded by ZonMW project No. 837002504; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, J.E.B., E.J.W.S., and P.S. declared no conflicts of interest, and A.S., J.L., and T.Z. had developed the online treatment and made the book version available online and in print but reported no commercial interests.
[Study 832] McCurry SM, Zhu W, Von Korff M, Wellman R, Morin CM, Thakral M, Yeung K, Vitiello MV. Effect of telephone cognitive behavioral therapy for insomnia in older adults with osteoarthritis pain: a randomized clinical trial. JAMA Internal Medicine. 2021;181(4):530-538. doi:10.1001/jamainternmed.2020.9049
Funding/Conflicts: Public Funding: From the study, the work was supported by Public Health Service grant 5R01AG053221 and National Institute on Aging grant R01AG053221; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source supported the study, but Dr Von Korff reported grants to Group Health Research Institute from Pfizer and Campbell Alliance Group, and Dr Morin reported grants from Idorsia and Canopy Health, consulting/advisory fees from Eisai, Merck, Pear Therapeutics, Sunovion, and Weight Watchers, and royalties from Mapi Research Trust outside the submitted work.
[Study 833] Wiklund T, Molander P, Lindner P, Andersson G, Gerdle B, Dragioti E. Internet-delivered cognitive behavioral therapy for insomnia comorbid with chronic pain: randomized controlled trial. Journal of Medical Internet Research. 2022;24(4):e29258. doi:10.2196/29258
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, the study stated that it received no funding, and the authors declared no conflicts of interest.
[Study 834] Zhang C, Liu Y, Guo X, Liu Y, Shen Y, Ma J. Digital cognitive behavioral therapy for insomnia using a smartphone application in China: a pilot randomized clinical trial. JAMA Network Open. 2023;6(3):e234866. doi:10.1001/jamanetworkopen.2023.4866
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, the work was funded by Shenzhen Zeen Health Technology, which also provided the Chinese version of the digital CBT-I app and smart bracelets for participants; the funder had no role in the study design, conduct, data collection, analysis, interpretation, manuscript preparation, review, approval, or decision to submit, and the authors reported no conflicts of interest.
[Study 835] Starling CM, Greenberg D, Lewin D, Shaw C, Zhou ES, Lieberman D, Chou J, Arem H. Voice-activated cognitive behavioral therapy for insomnia: a randomized clinical trial. JAMA Network Open. 2024;7(9):e2435011. doi:10.1001/jamanetworkopen.2024.35011
Funding/Conflicts: Public Funding: From the study, the work was supported by National Cancer Institute grant R44CA232905, and the NCI had no role in the study design, conduct, data collection, management, analysis, interpretation, manuscript preparation, review, approval, or decision to submit; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, Dr. Lewin reported grants from the Sleep Health and Wellness Center during the study, Prof. Arem reported NCI grants during the study and funding from the Maryland Department of Health and the Centers for Disease Control and Prevention outside the submitted work, and no other disclosures were reported.
[Study 836] Malarkey ME, Fu AJ, Mannan N, Shaw OM, Haight TJ, Cota MR, Jahed NC, Werner JK, Brody DL. Internet-guided cognitive behavioral therapy for insomnia among patients with traumatic brain injury: a randomized clinical trial. JAMA Network Open. 2024;7(7):e2420090. doi:10.1001/jamanetworkopen.2024.20090
Funding/Conflicts: Public Funding: From the study, the work was supported by the Uniformed Services University Military Traumatic Brain Injury Initiative, formerly known as the Center for Neuroscience and Regenerative Medicine; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, but Dr. Brody disclosed outside-the-submitted-work consulting for QualWorld, Cirrito Holdings LLC, and Algernon Pharmaceuticals Inc., royalties from Oxford University Press, grant funding from the US Department of Defense and NIH, and service as editor-in-chief of the Journal of Neurotrauma; no other disclosures were reported.
[Study 837] Ritterband LM, Shaffer KM, Thorndike FP, Chow PI, Gonder-Frederick L, Ingersoll KS, Cohn WF, Frederick C, MacDonnell K, Glazer JV, Mattos MK, Hilgart MM, Quigg MS, Bashir M, Morin CM. A randomized controlled trial of a digital cognitive behavioral therapy for insomnia for older adults. NPJ Digital Medicine. 2025;8:458. doi:10.1038/s41746-025-01847-0
Funding/Conflicts: Public Funding: From the study, the trial was funded by the National Institutes of Health/National Institute on Aging grant R01AG047885; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, but L.M.R., F.P.T., L.G.-F., and C.M.M. reported equity ownership in BeHealth Solutions, LLC; F.P.T. was an employee of Nox Health, which owns the IP of Somryst; L.M.R. and C.M.M. were paid consultants of Nox Health; C.M.M. also reported advisory/consulting roles and research support from several companies, and the article states these companies had no role in manuscript preparation.