
Doctor explains why Retatutride is the BEST Fat Loss Peptide

Main Points
Claim: Retatrutide reduces insulin resistance and increases metabolism as a person loses weight.
Conclusion: The insulin-resistance part is strongly supported. Retatrutide lowers HbA1c and improves blood sugar control. The metabolism part is promising but not yet proven in humans. The best conclusion is that retatrutide clearly improves insulin resistance and may help preserve metabolism during weight loss.
Claim: GLP-1 works by reducing hunger, but has the consequences of constipation and nausea.
Conclusion: This claim is well supported. GLP-1-based drugs reduce hunger by acting on brain pathways that increase fullness. Nausea, gastrointestinal discomfort, and constipation are recognized side effects. The conclusion is that these drugs help control appetite, but digestive issues are part of the tradeoff.
Claim: Tirzepatide is better, because it dampens nausea and leads to more weight loss.
Conclusion: The weight-loss part is supported, but the nausea claim is less clear. Tirzepatide appears to produce more weight loss than semaglutide, but it does not clearly cause fewer side effects and may cause slightly more at higher doses. The conclusion is that tirzepatide is better for weight loss, though not necessarily easier to tolerate.
Claim: Retatrutide includes glucagon receptor agonism to increase lipolysis and resting metabolism.
Conclusion: This claim is supported by preclinical evidence. Blocking the glucagon receptor makes retatrutide less effective, suggesting this pathway adds to its fat-loss and metabolism effects. The conclusion is that glucagon receptor agonism likely gives retatrutide an advantage, though stronger human evidence is still needed.
The algorithms have done it again and introduced me to yet another health creator, this time Dr. Ashley Froese, a physician and health educator who focuses heavily on biohacking tools.
In this discussion, the focus is on why the peptide retatrutide may be such a powerful treatment for obesity and metabolic health. To sort through that idea properly, it helps to take each major claim one at a time and compare it against the evidence.
The main claims are these:
Retatrutide reduce Insulin Resistance and increases Metabolism as a person Loses Weight
GLP-1 peptides work through reducing hunger, but has consequences of constipation and nausea
Tirzepatide is better, because it dampens nausea and leads to more weight loss
Retatrutide is even better, because it has specialized effects
Claim 1: Retatutride reduces Insulin Resistance and raises Metabolism
The first claim is that retatrutide improves insulin resistance, which is the underlying problem that drives much of type 2 diabetes. On this point, the evidence is strong.
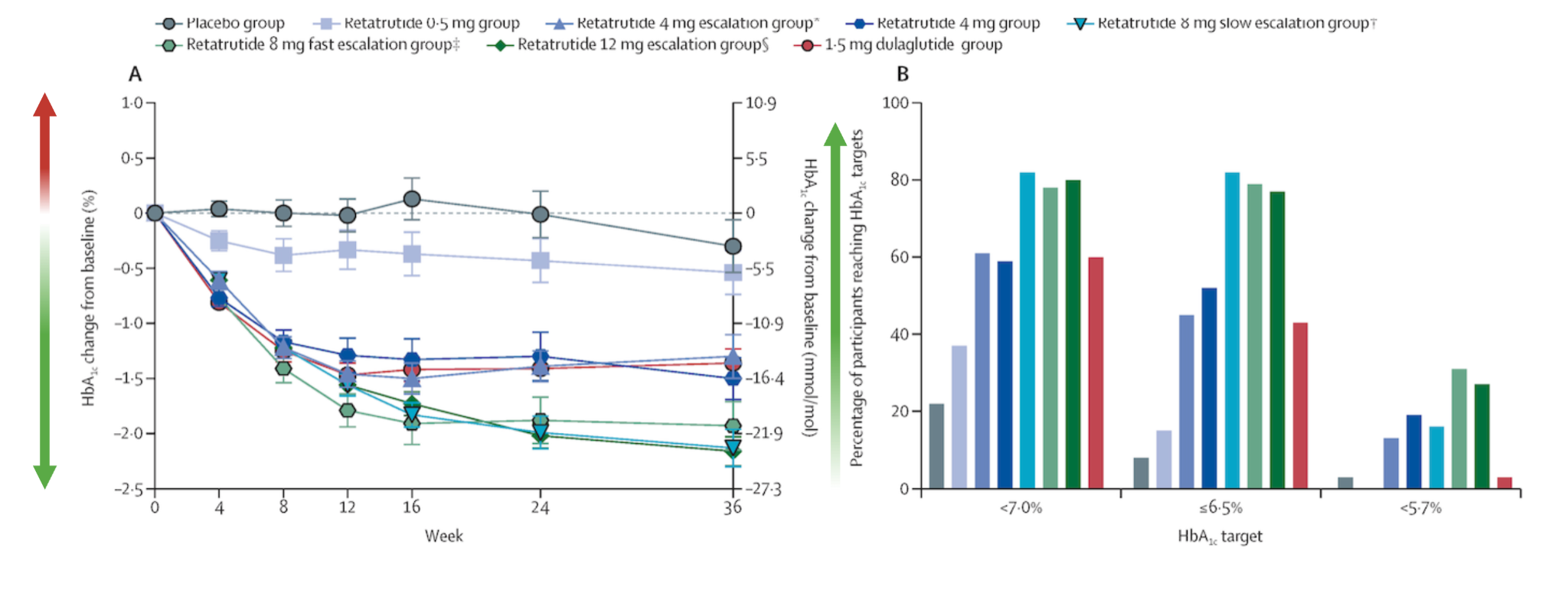
One clinical study was designed to examine exactly this issue [1]. The researchers used several dosing strategies for retatrutide and measured HbA1c, also called glycated hemoglobin. HbA1c is a long-term marker of blood sugar control.
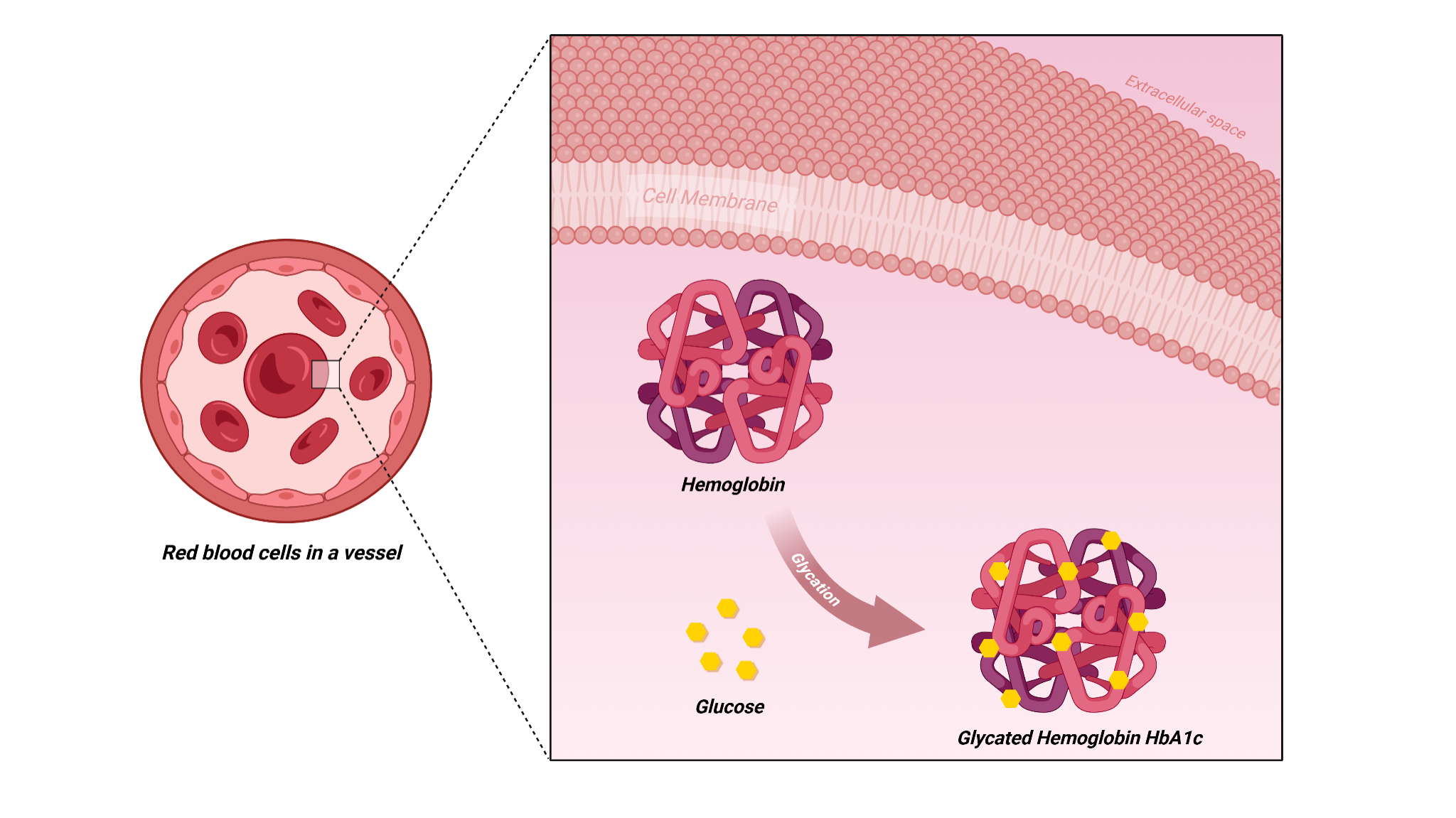
It reflects how much sugar has attached to proteins in red blood cells over time. When HbA1c is too high, it usually means blood sugar has been elevated for a prolonged period, which strongly suggests insulin resistance.
In the study, people with significant insulin resistance experienced reductions in HbA1c across retatrutide doses, with stronger effects at higher doses. A large proportion of participants at the higher doses achieved major improvements in HbA1c, including movement toward normalized values. That makes the conclusion fairly straightforward: retatrutide appears to be highly effective for improving insulin resistance.
So, the point here is that Dr. Ashley is absolutely right - retatrutide is highly effective against insulin resistance.
The second part of that first claim is that retatrutide increases metabolism as a person loses weight. This idea is more uncertain.
Metabolism, in this context, refers to the body’s energy expenditure, meaning how much energy the body uses to maintain its normal functions and support activity. One of the classic problems with weight loss is that when calories fall, the body often adapts by lowering energy expenditure. This makes continued fat loss harder over time.
As far as the evidence discussed here goes, there are no direct human studies clearly showing that retatrutide raises metabolism during weight loss.
Researchers have suggested this may happen, but the clearest support comes from animal studies [2]. In those studies, retatrutide appeared to maintain energy expenditure better than calorie restriction alone, even when food intake was matched. At the same time, the animals given retatrutide lost more weight than animals who simply ate less.
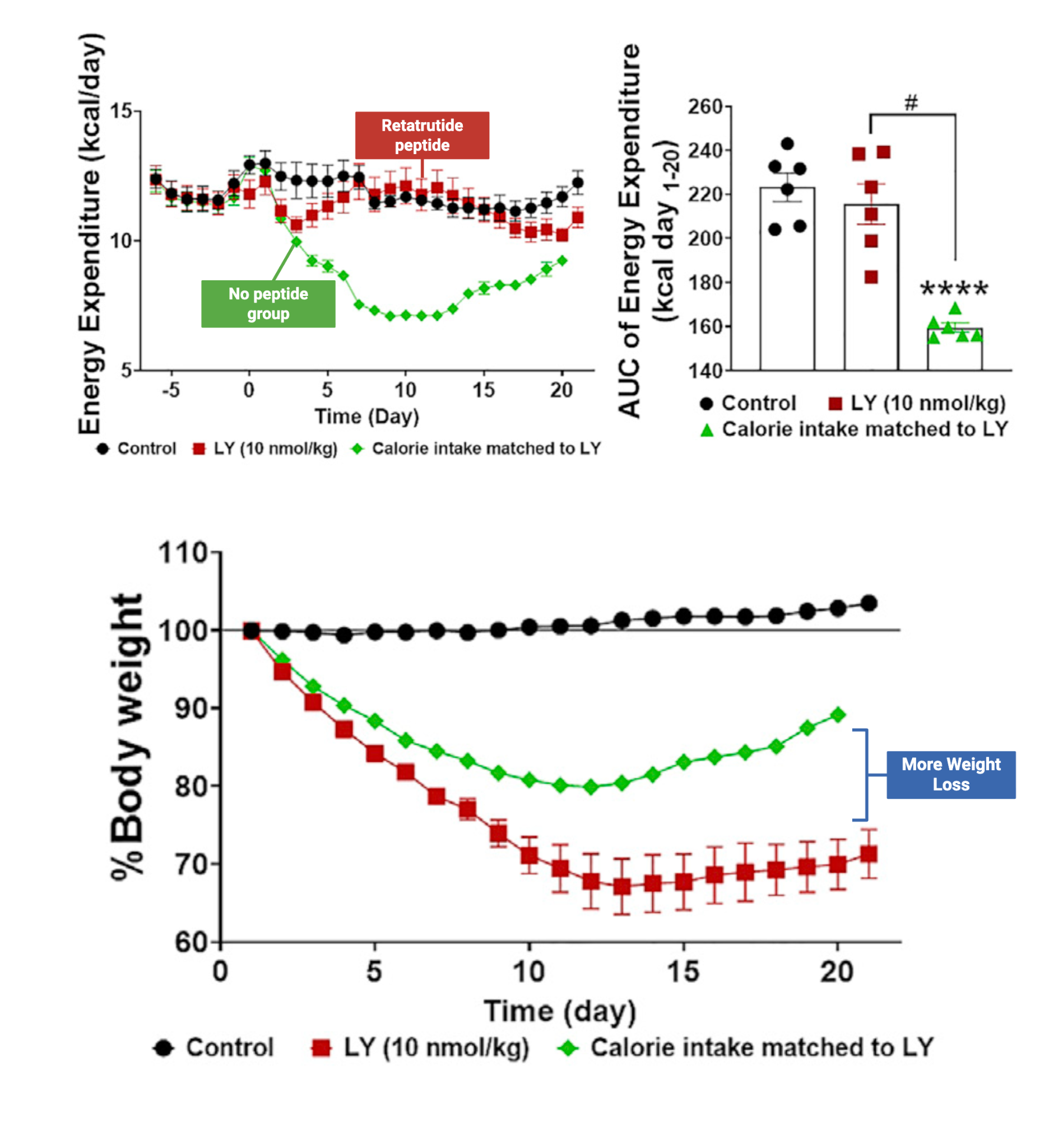
That combination is important. It suggests the drug may be doing more than suppressing appetite. It may also help prevent the usual metabolic slowdown that comes with dieting. Still, because this evidence is preclinical rather than directly demonstrated in humans, the confidence level is lower.
The main point here is that it is likely that retatrutide boosts metabolism even when the body is chronically exposed to a calorie-restricted diet, but the evidence is not shown in humans, yet, so the certainty is lower than for the insulin resistance data.
Claim 2: GLP-1 peptides work by reducing hunger, but have consequences of constipation and nausea
The next claim is that GLP-1 peptides work by reducing hunger. This is well supported.
GLP-1 stands for glucagon-like peptide-1 [4], which is a hormone involved in blood sugar control, digestion, and appetite regulation. GLP-1-based drugs bind to receptors in the brain and influence neurons, which are nerve cells, in ways that reduce hunger signals and increase fullness.
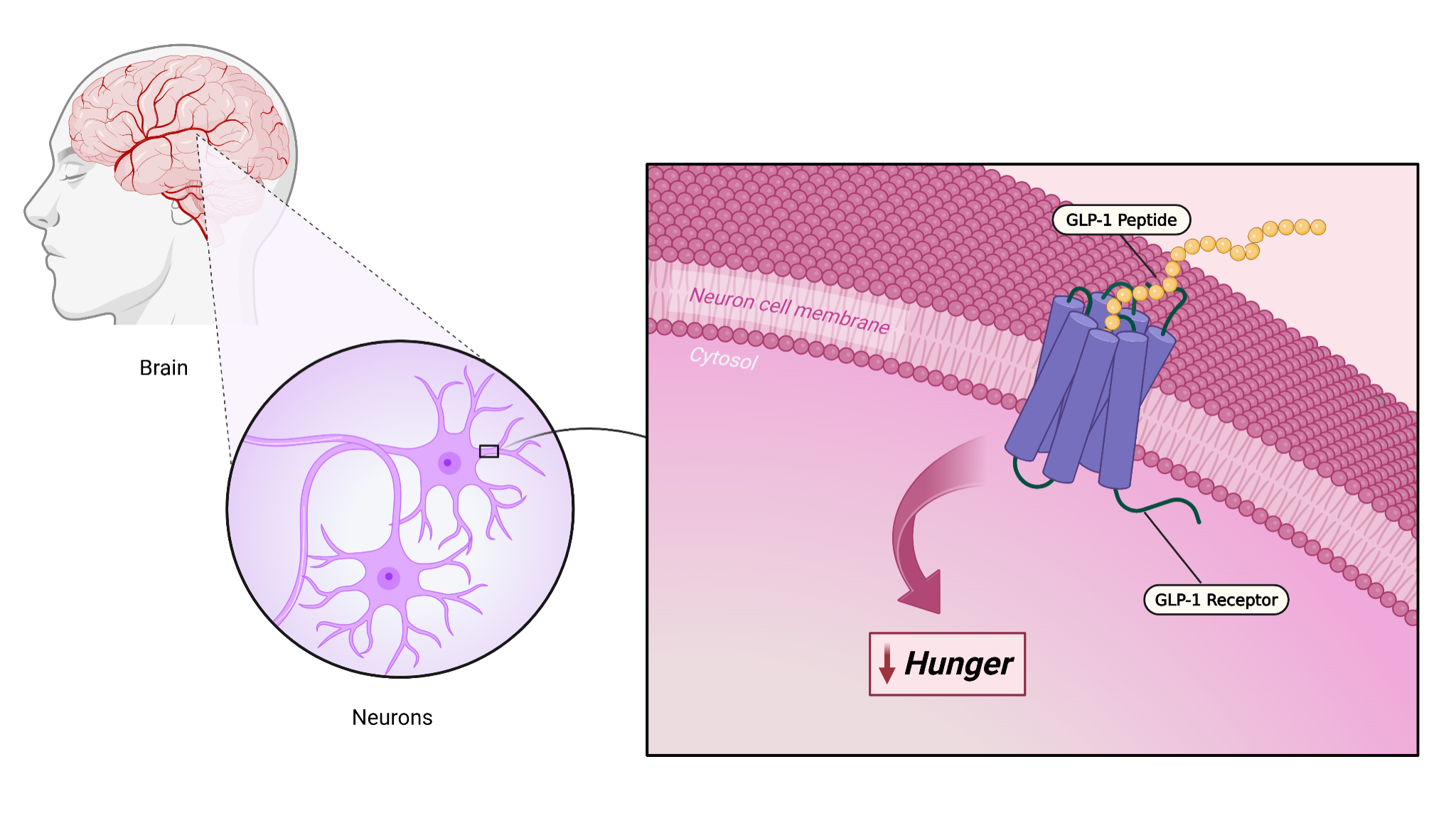
One interesting (and funny) detail is the involvement of a gene pathway called CART, which stands for cocaine- and amphetamine-regulated transcript.
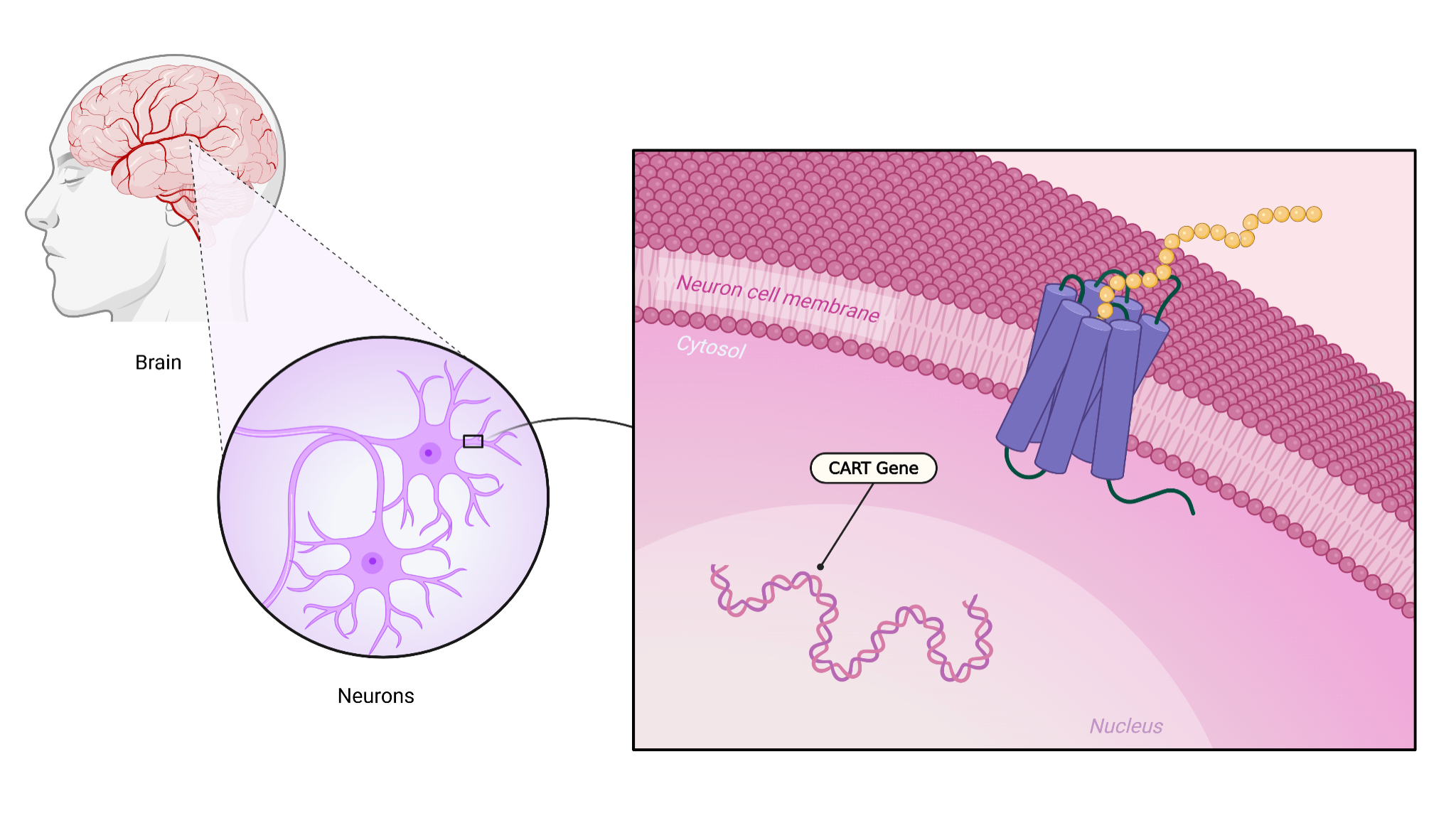
The name sounds unusual, but the key idea is simple: activation of this pathway is associated with reduced hunger. When GLP-1 signaling increases, this can help push the brain toward a state where appetite is reduced.
So, on the basic mechanism, GLP1 peptides typically work through reducing hunger, and yes, they are prone to gastrointestinal side effects.
Nausea and Constipation Are Real Tradeoffs
The same claim also states that GLP-1 peptides can cause constipation and nausea. That is also true.
Reviews of GLP-1 drugs describe gastrointestinal side effects as one of the main drawbacks. Nausea is especially common, and constipation or general gastrointestinal discomfort can occur as well. These effects do not happen to everyone, and their intensity can vary, but they are established side effects rather than rare or speculative concerns.
So the short version is simple: GLP-1 peptides help reduce hunger, but digestive side effects are part of the tradeoff.
Claim 3: Tirzepatide is better because it dampens nausea and leads to more weight loss
The next claim is that tirzepatide is better because it leads to more weight loss. On this point, the evidence supports the claim.
Because tirzepatide has been studied directly against GLP-1 receptor agonists such as semaglutide, researchers [5] have been able to compare outcomes. In those comparisons, tirzepatide produces greater weight loss. Much of that loss appears to be fat loss, which is one reason the drug has attracted so much attention.
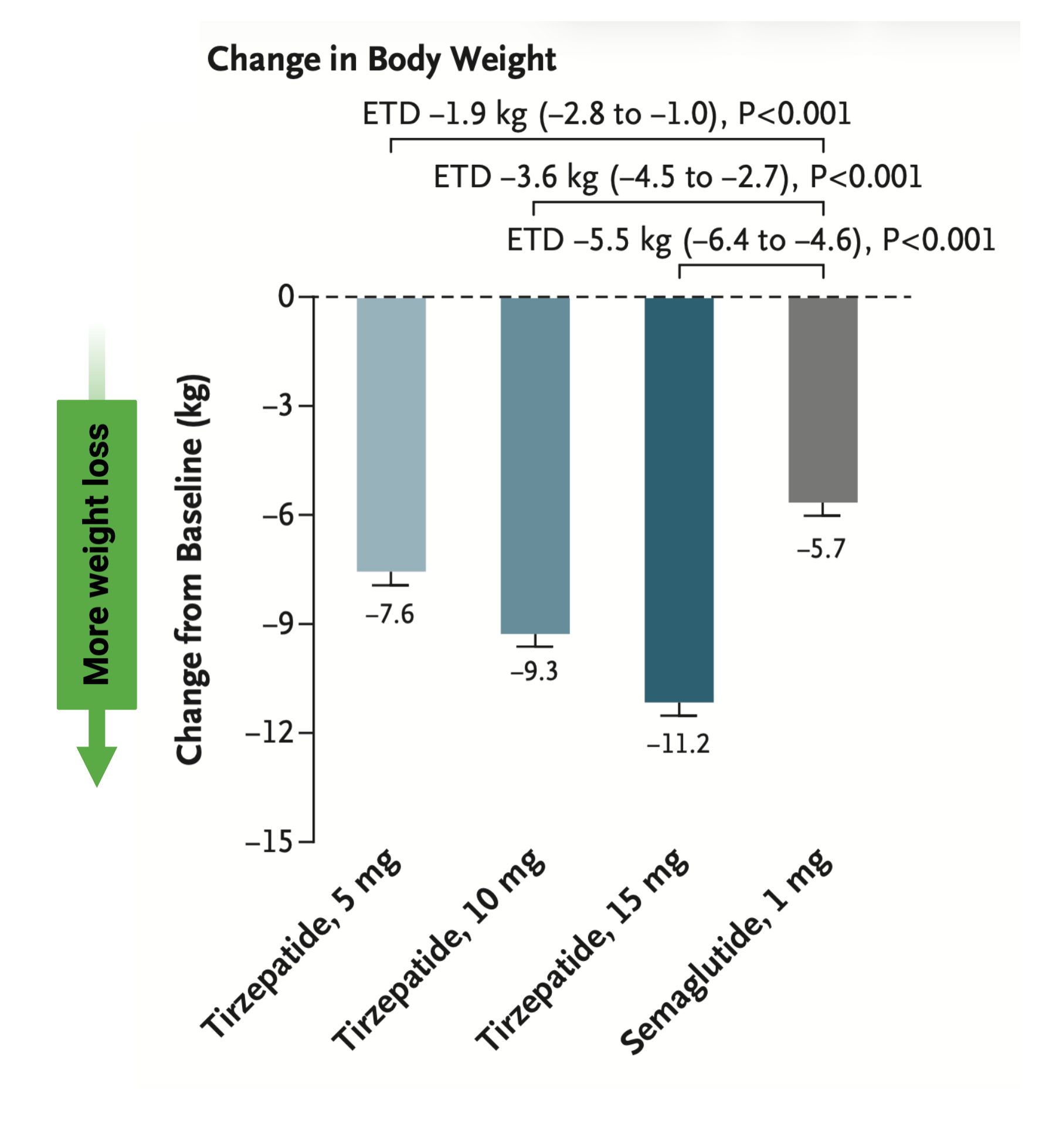
That means the broad claim that tirzepatide is more effective for weight loss than a standard GLP-1 peptide (semaglutide) is well supported.
The Nausea Advantage Is Less Clear
The harder part of the tirzepatide claim is the idea that it dampens nausea or causes fewer side effects.
Here the evidence is less favorable. In the comparison discussed, tirzepatide did not clearly show fewer side effects overall than semaglutide. At higher doses, tirzepatide actually showed a slightly higher proportion of side effects. That means it is not accurate to say, in a blanket way, that tirzepatide is simply easier to tolerate.
There are a few important things to consider. One, the people in the study had type 2 diabetes, so the results may not apply perfectly to every population. Also, the side-effect differences were not massive, which is further confirmed in analyses of many studies [6].
So, the point here being that tirzepatide is better for fat loss, but at higher doses does yield more side effects. If using a comparable dose to a GLP-1 receptor agonist peptide alone, you’ll likely get more results with similar side effects.
Peptides and the ‘Futile Calcium Cycle’
Peptides and Brown Fat Activation
Peptides and Uncoupling Mitochondria
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
Retatrutide’s Glucagon Receptor Effect May Give It an Edge
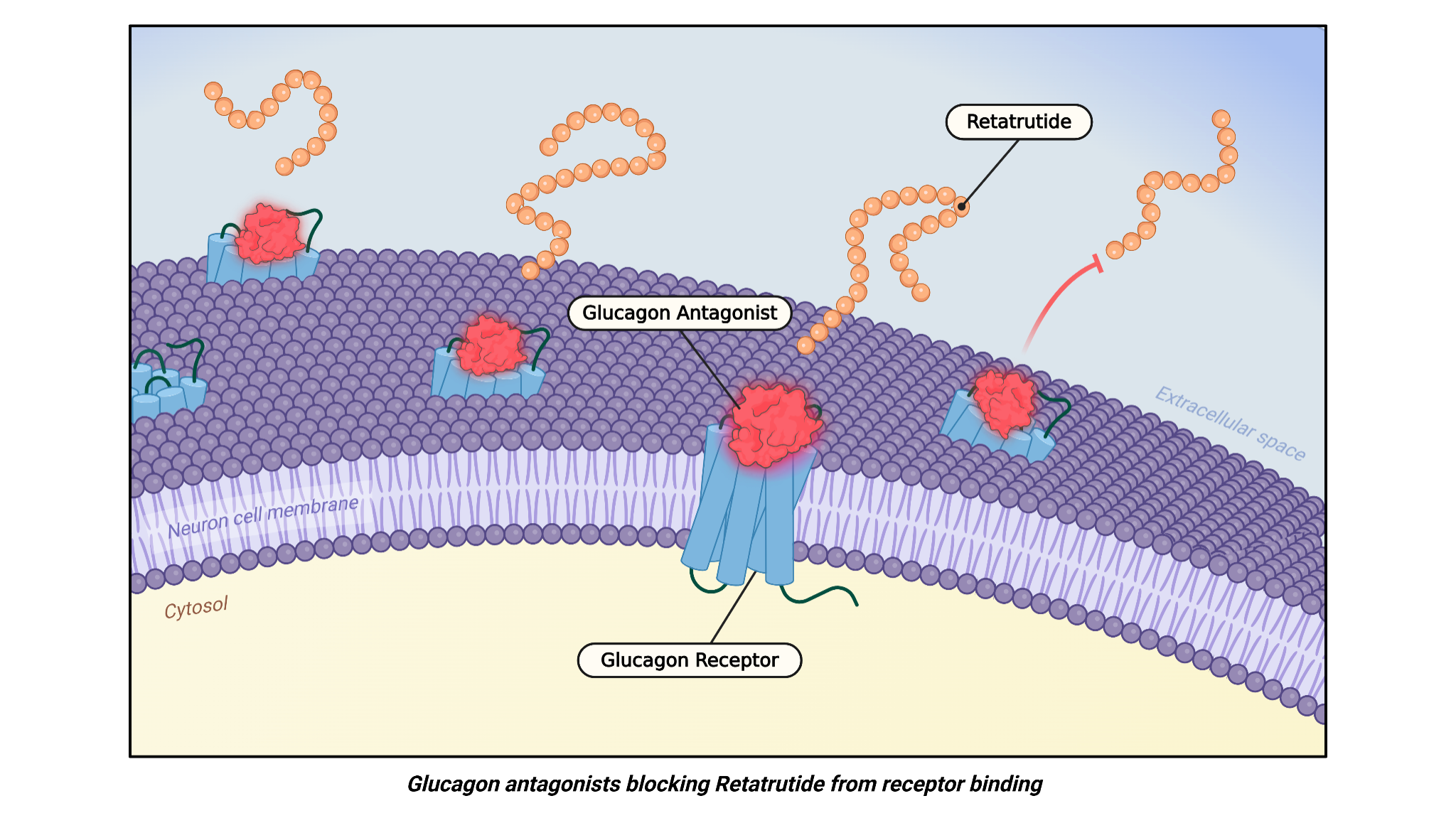
The next claim is that retatrutide includes glucagon receptor agonism to increase fat loss and metabolism. This is one of the most interesting parts of the retatrutide story.
An agonist is something that activates a receptor. Retatrutide is notable because it activates not just GLP-1 and GIP pathways, but also the glucagon receptor. Glucagon is often thought of as a hormone involved in raising blood sugar, but it also appears to play a role in energy expenditure and fat metabolism.
The key evidence discussed here comes from animal studies [3] in which researchers isolated the glucagon-related effects from the rest of the peptide. When they blocked the glucagon receptor, retatrutide became less effective. It did not stop working entirely, which means the other receptor actions still mattered, but the loss of some benefit strongly suggests that glucagon receptor activation contributes meaningfully to the overall fat-loss effect.
The same pattern appears in the metabolism data. Retatrutide helped maintain energy expenditure, but when glucagon receptors were blocked, that effect was weaker (seen in the figure below). This points to the glucagon part of the molecule as an important contributor to its metabolic advantage.
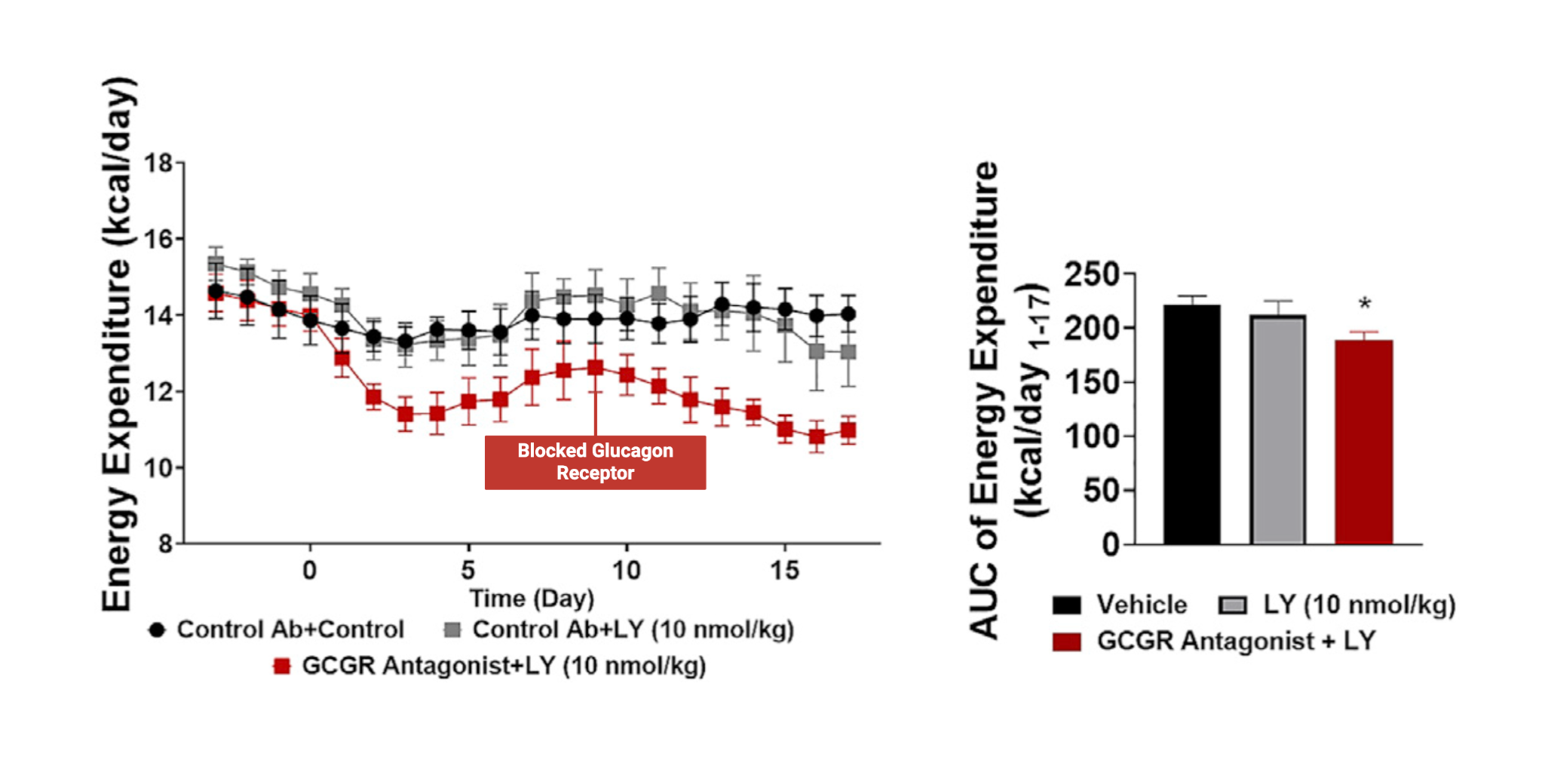
This does not mean every detail is fully proven in humans. It does mean there is a strong mechanistic case that glucagon receptor agonism helps explain why retatrutide may outperform simpler peptide designs.
Side Effects Still Matter
A few final points help put the larger picture into context.
One issue is lean mass loss. Lean mass is often described casually as muscle, but that is not technically precise. Lean mass includes muscle, but it also includes other components such as glycogen, which is stored carbohydrate, along with the water associated with it. Since weight loss usually lowers glycogen stores, a reduction in lean mass does not automatically prove direct muscle loss. Muscle loss is certainly possible, but the more careful claim is that some lean mass loss can occur.
Other side effects mentioned include a slight increase in heart rate and a mild burning sensation in the skin for some people. These effects are worth noting, but they do not undo the broader conclusion that these peptides can be effective tools for fat loss and metabolic improvement.
Where the Evidence Leaves Us
Taken together, the overall picture is fairly clear. GLP-1 receptor agonists such as semaglutide are effective for fat loss. Tirzepatide appears more effective than a standard GLP-1 agonist, especially for weight reduction. Retatrutide may be more effective still, partly because it includes glucagon receptor agonism, which may help it preserve metabolism during a calorie deficit and enhance fat loss through mechanisms beyond appetite suppression alone.
At the same time, side effects remain part of the story for all of these drugs. The percentage of people who experience side effects is not overwhelming, but the side effects are real and should not be ignored. The strongest claims for retatrutide involve insulin resistance and overall weight-loss potential. The most intriguing claims, especially around metabolism, are promising but still depend heavily on early mechanistic and preclinical work.
Main Points
Claim: Retatrutide reduces insulin resistance and increases metabolism as a person loses weight.
Conclusion: The insulin-resistance part is strongly supported. Retatrutide lowers HbA1c and improves blood sugar control. The metabolism part is promising but not yet proven in humans. The best conclusion is that retatrutide clearly improves insulin resistance and may help preserve metabolism during weight loss.
Claim: GLP-1 works by reducing hunger, but has the consequences of constipation and nausea.
Conclusion: This claim is well supported. GLP-1-based drugs reduce hunger by acting on brain pathways that increase fullness. Nausea, gastrointestinal discomfort, and constipation are recognized side effects. The conclusion is that these drugs help control appetite, but digestive issues are part of the tradeoff.
Claim: Tirzepatide is better, because it dampens nausea and leads to more weight loss.
Conclusion: The weight-loss part is supported, but the nausea claim is less clear. Tirzepatide appears to produce more weight loss than semaglutide, but it does not clearly cause fewer side effects and may cause slightly more at higher doses. The conclusion is that tirzepatide is better for weight loss, though not necessarily easier to tolerate.
Claim: Retatrutide includes glucagon receptor agonism to increase lipolysis and resting metabolism.
Conclusion: This claim is supported by preclinical evidence. Blocking the glucagon receptor makes retatrutide less effective, suggesting this pathway adds to its fat-loss and metabolism effects. The conclusion is that glucagon receptor agonism likely gives retatrutide an advantage, though stronger human evidence is still needed.
Peptides and the ‘Futile Calcium Cycle’
Peptides and Brown Fat Activation
Peptides and Uncoupling Mitochondria
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
Dr. Nicolas Verhoeven, PhD / Physionic
References
[1] Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA. Lancet. 2023;402(10401):529-544. doi:10.1016/S0140-6736(23)01053-X
[2] Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. doi:10.1056/NEJMoa2301972
[3] Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept. Cell Metab. 2022;34(9):1234-1247.e9. doi:10.1016/j.cmet.2022.07.013
[4] Drucker DJ. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018;27(4):740-756. doi:10.1016/j.cmet.2018.03.001
[5] Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385(6):503-515. doi:10.1056/NEJMoa2107519
[6] Karagiannis T, Malandris K, Avgerinos I, et al. Subcutaneously administered tirzepatide vs semaglutide for adults with type 2 diabetes: a systematic review and network meta-analysis of randomised controlled trials. Diabetologia. 2024;67(7):1206-1222. doi:10.1007/s00125-024-06144-1
[7] Yu X, Chen S, Funcke JB, et al. The GIP receptor activates futile calcium cycling in white adipose tissue to increase energy expenditure and drive weight loss in mice. Cell Metab. 2025;37(1):187-204.e7. doi:10.1016/j.cmet.2024.11.003
[8] Zhang A, Liu Q, Xiong Y, et al. Tirzepatide reduces body weight by increasing fat utilization via the central nervous system-adipose tissue axis in male mice. Diabetes Obes Metab. 2025;27(5):2844-2856. doi:10.1111/dom.16294
[9] Salem V, Izzi-Engbeaya C, Coello C, et al. Glucagon increases energy expenditure independently of brown adipose tissue activation in humans. Diabetes Obes Metab. 2016;18(1):72-81. doi:10.1111/dom.12585