
This New GLP-1 Study Changes the Muscle Loss Debate

Main Points
Weight-loss peptides can lead to lean mass loss, and muscle is a major part of lean mass. Direct muscle weighing in animal research also shows reductions in muscle mass.
However, absolute muscle loss does not tell the full story. When muscle mass is measured relative to total bodyweight, the peptide condition does not show a disproportionate loss of muscle. This suggests the muscle-loss concern may be overstated when the data are interpreted only through absolute values.
Muscle function also appears to follow a similar pattern. Absolute force may decline, but relative force generation is not especially worsened by peptide use after accounting for bodyweight changes.
Peptides do not appear to cause a special muscle-loss effect that is clearly separate from calorie restriction. Both calorie restriction and peptide use lead to similar lean mass and muscle mass losses when exercise is not added.
Early human evidence with semaglutide shows the same general pattern: absolute muscle mass may decrease, but relative muscle mass and function do not appear to be meaningfully worsened.
Overall, weight loss can reduce muscle mass and function, but peptides appear to mostly drive fat loss, with smaller muscle-related losses that are not unique to peptide use. Pairing weight loss with resistance training would likely make muscle preservation even more favorable.
One of the scariest concerns that comes with popular fat-loss peptides, like semaglutide, tirzepatide, and newer related peptides, is muscle loss.
Muscle is a form of lean tissue with major metabolic and functional benefits. It helps regulate blood sugar and insulin by taking up blood sugar, but it also allows us to move, stabilize ourselves, catch ourselves from falls, and maintain physical freedom in daily life.
These peptides can be very effective for weight loss and, admittedly, fat loss. But the key concern is whether that weight loss also comes with muscle loss.
The Lean Mass Loss Concern
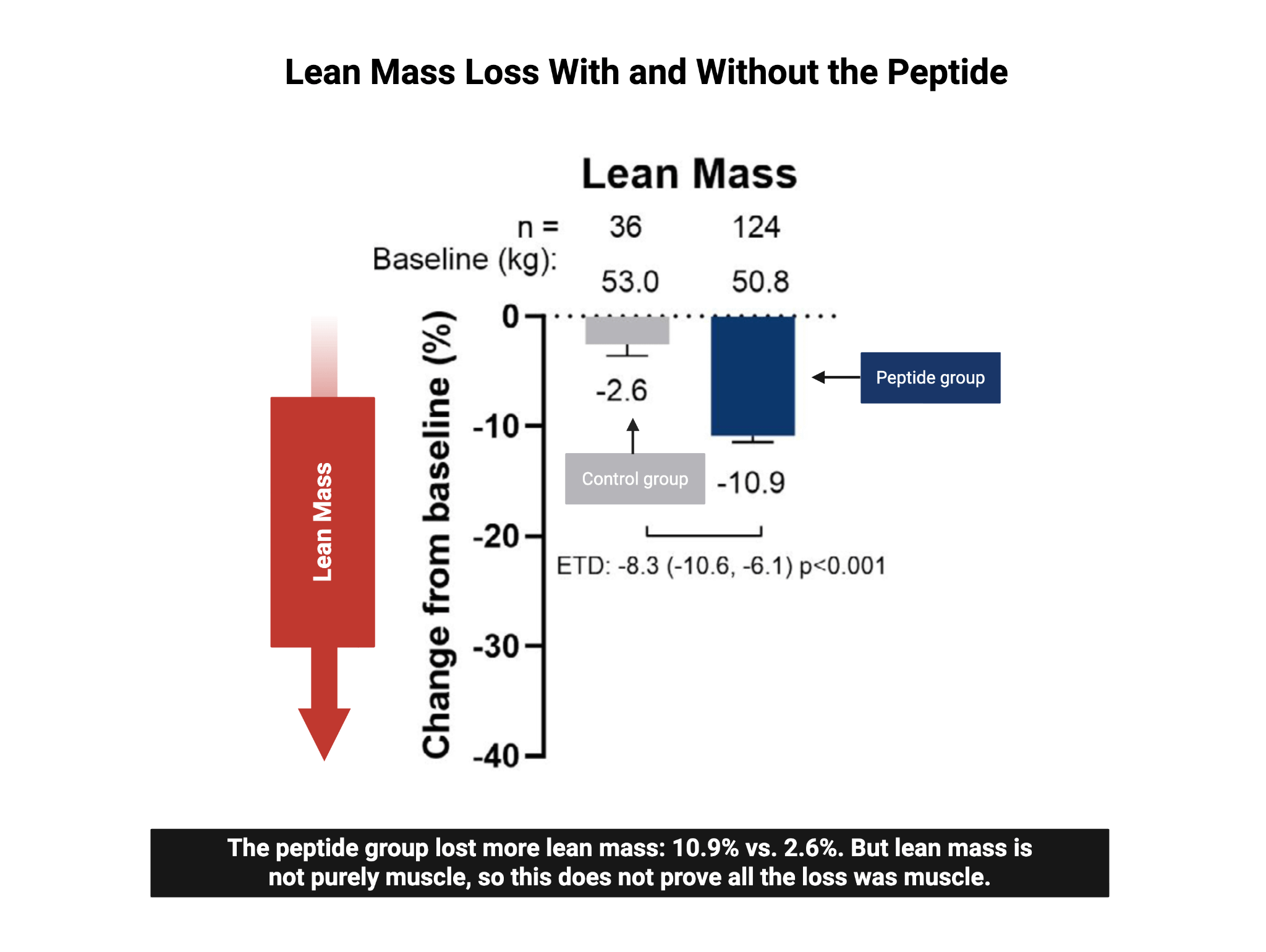
The concern comes from human data [780] showing that people using one of these peptides experienced much greater lean mass loss compared with those not using the peptide. Lean mass is not the same thing as muscle, but muscle is a major component of lean mass.
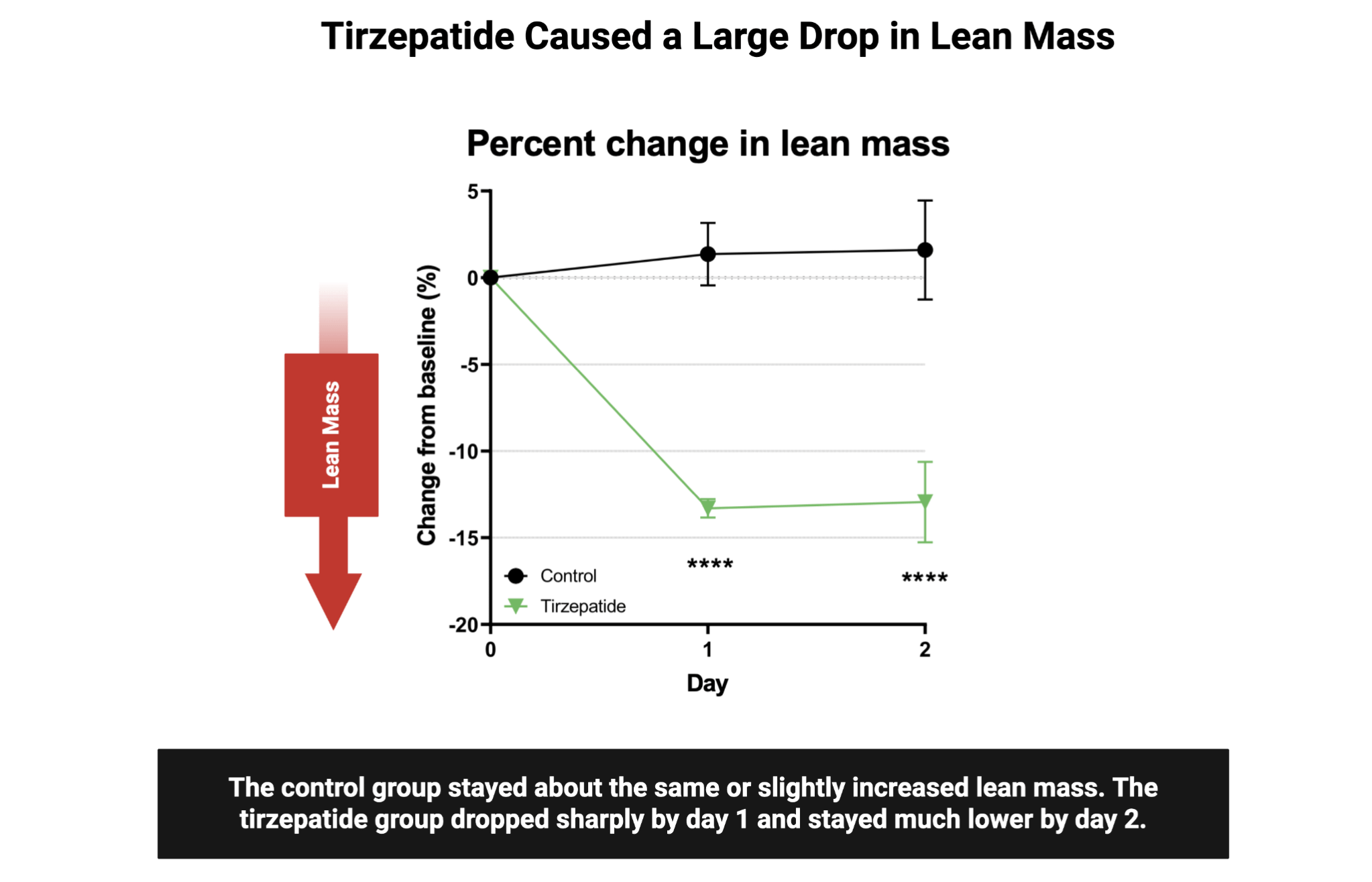
That pattern has also been repeated in a recent study [777], including animal research, where the peptide intervention again showed clear reductions in lean mass.
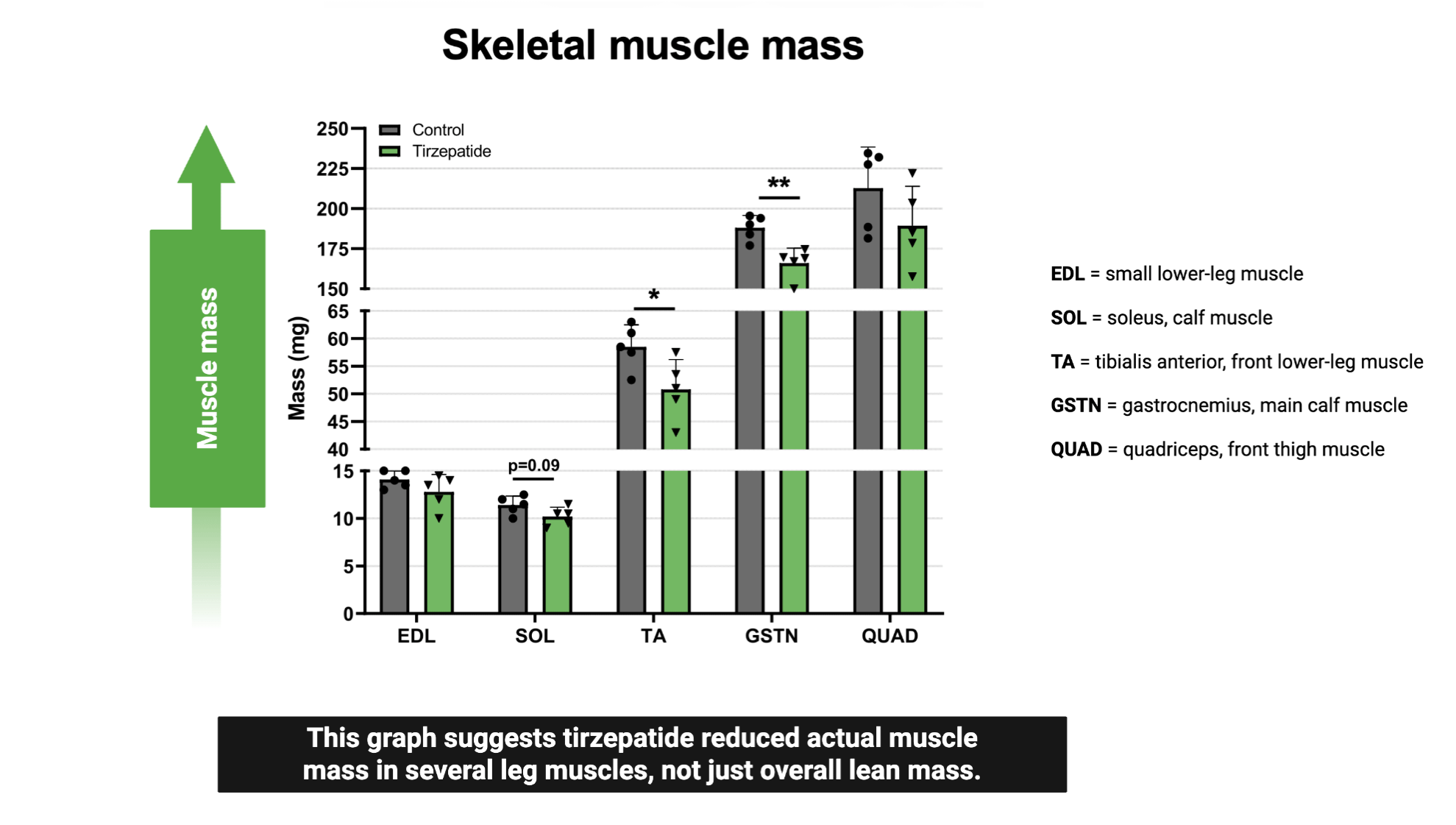
When muscle mass was measured directly across several leg muscles, the peptide-treated condition generally showed reductions in muscle mass. So, at first glance, the obvious conclusion seems to be that peptides like tirzepatide and semaglutide lead to lean mass loss and even a loss of muscle mass when measured directly.
Why Absolute Muscle Loss Does Not Tell the Whole Story
At this point, it may seem like the case is closed: peptides cause muscle loss.
But the way these data are collected matters. A major issue is that some of the data are based on absolute values. In other words, the muscle is removed and weighed as-is.
From that absolute weight perspective, yes, there is a reduction in muscle mass.
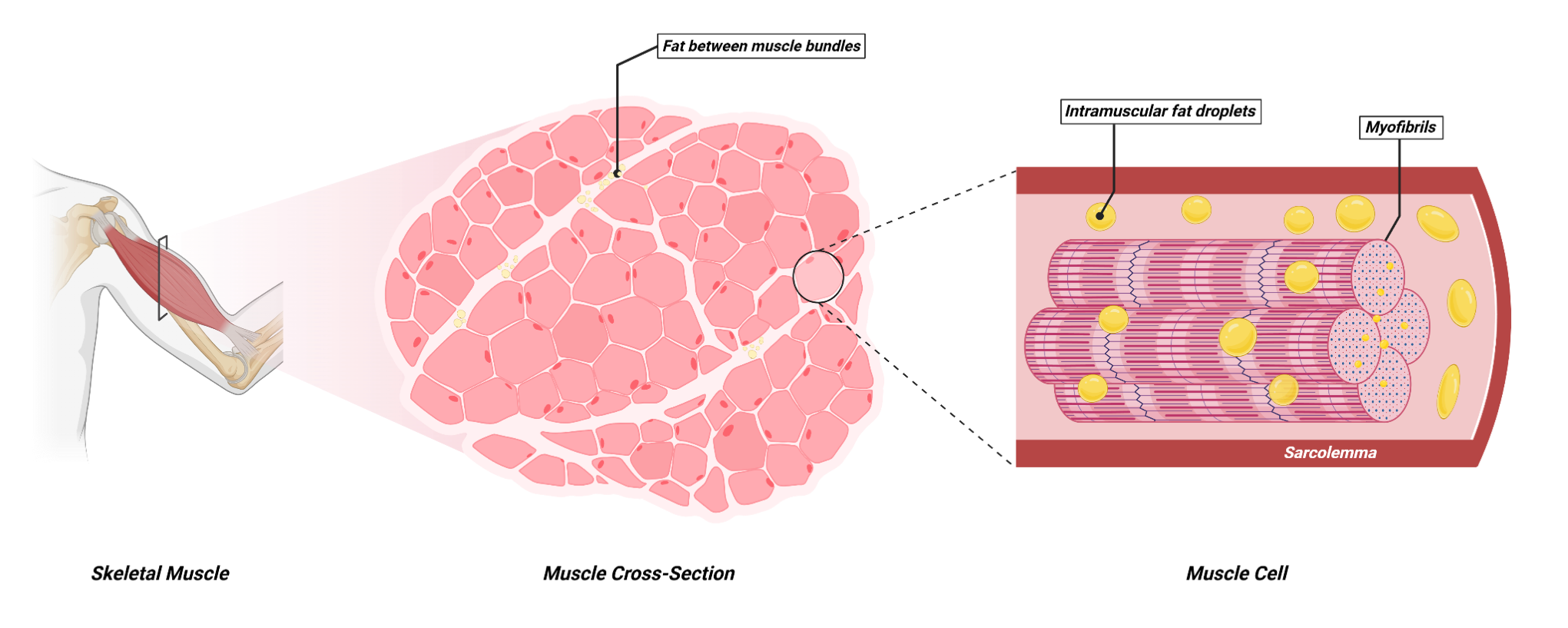
But that does not automatically mean the muscle tissue itself is disappearing. Muscle can also contain fat, both inside muscle cells and around muscle cells. So, it is possible for muscle weight to decrease partly because of changes in fat stored within or around the muscle, not necessarily because the actual contractile muscle tissue is being uniquely destroyed.
Relative Muscle Mass Changes the Interpretation
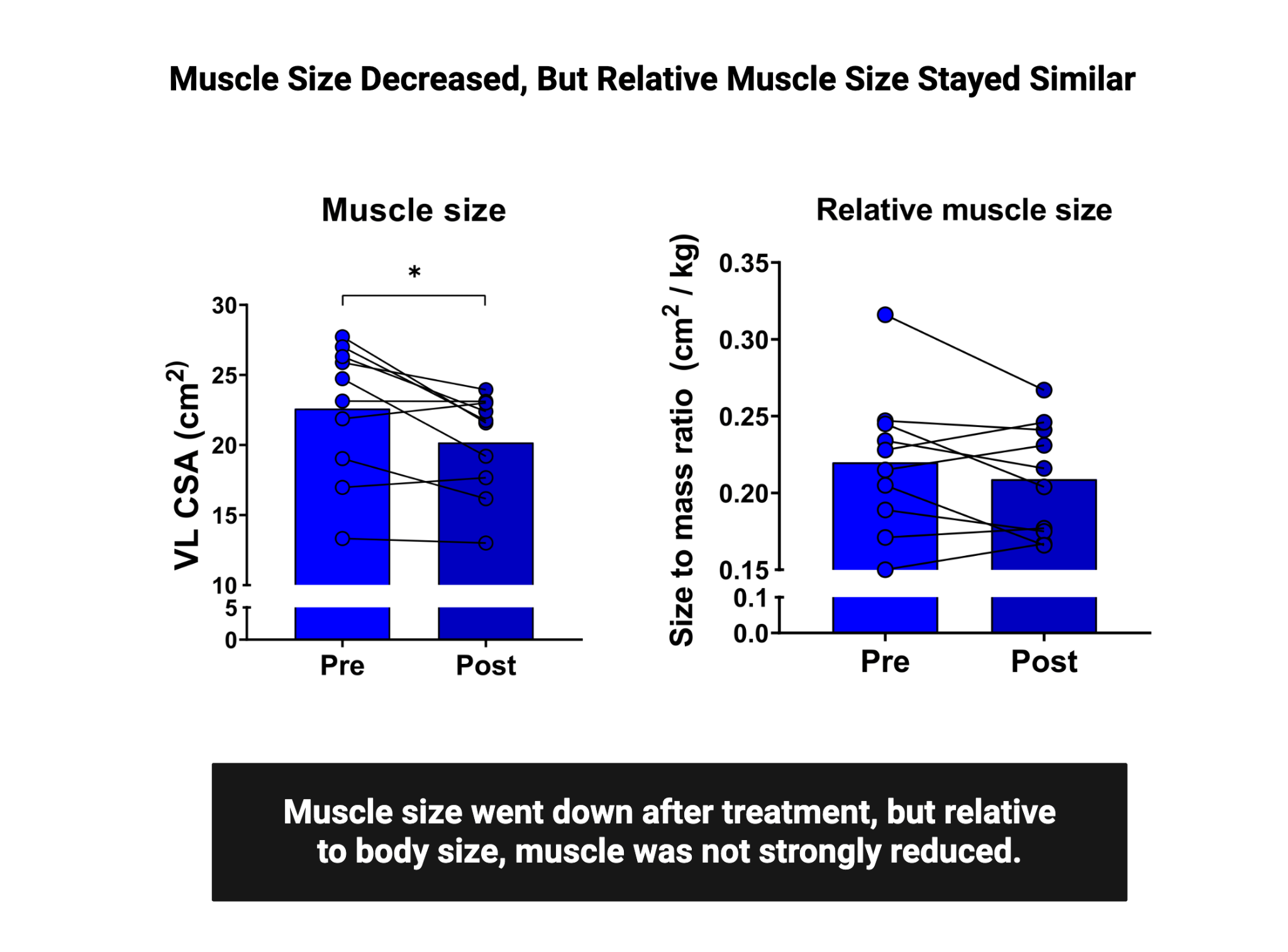
The next important question is what happens when muscle mass is measured relative to total bodyweight.
That matters because if total bodyweight drops substantially, some reduction in absolute muscle weight may be expected. The real concern is whether muscle is being lost disproportionately compared with the rest of the body.
When muscle mass was measured relative to bodyweight, the peptide-treated group actually showed an increase compared with the control group.
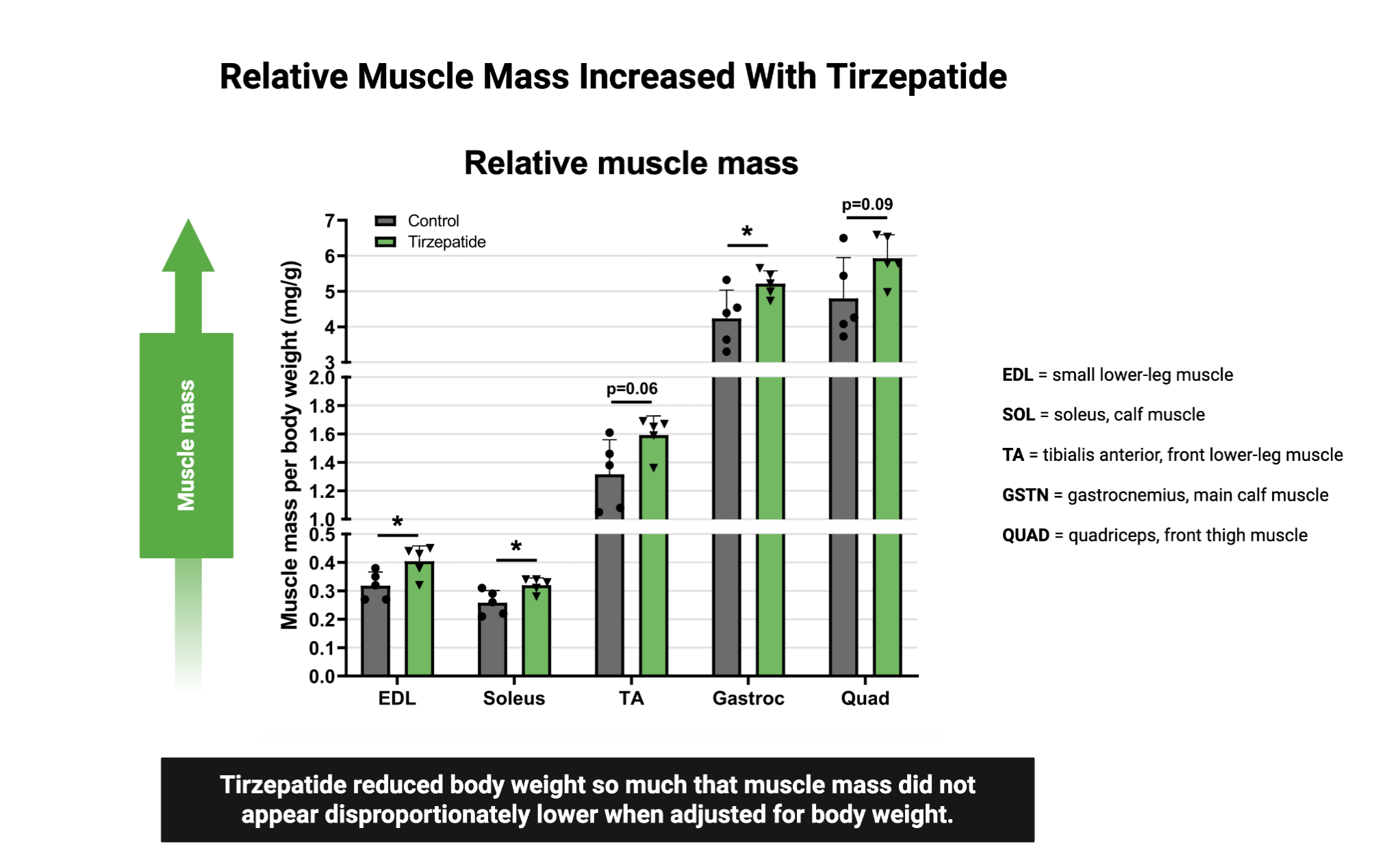
That flips the interpretation. It suggests that the muscle is not being disproportionately affected by peptide use. If muscles were only measured in absolute terms, the conclusion would look much worse. But when muscle is compared with total bodyweight, the data suggest that muscle is being maintained relatively well.
So, maybe muscle is not directly compromised by these peptides in the way people fear. However, much of this evidence still comes from mice, and muscle size is not the only issue. Muscle function may matter even more.
Peptides versus Dieting: Greater Risk of Lean Mass Loss?
An Odd Muscle Weakening and Rebounding Effect
Peptides on Muscle Mitochondria
Are Older People more likely to lose Lean Mass?
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
Muscle Function Matters More Than Size Alone
Retaining muscle size relative to bodyweight matters, but it does not automatically mean the muscle functions just as well.
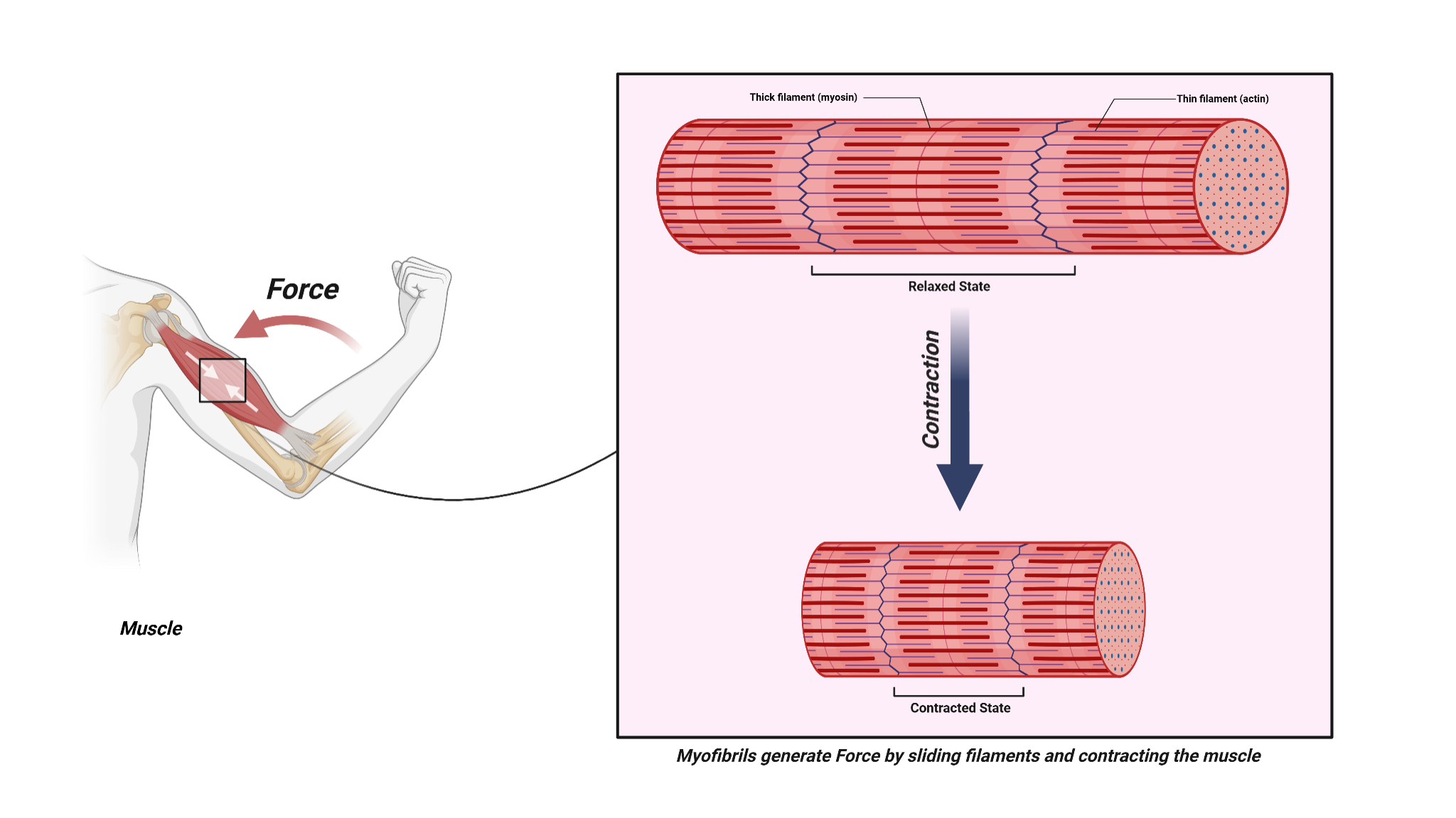
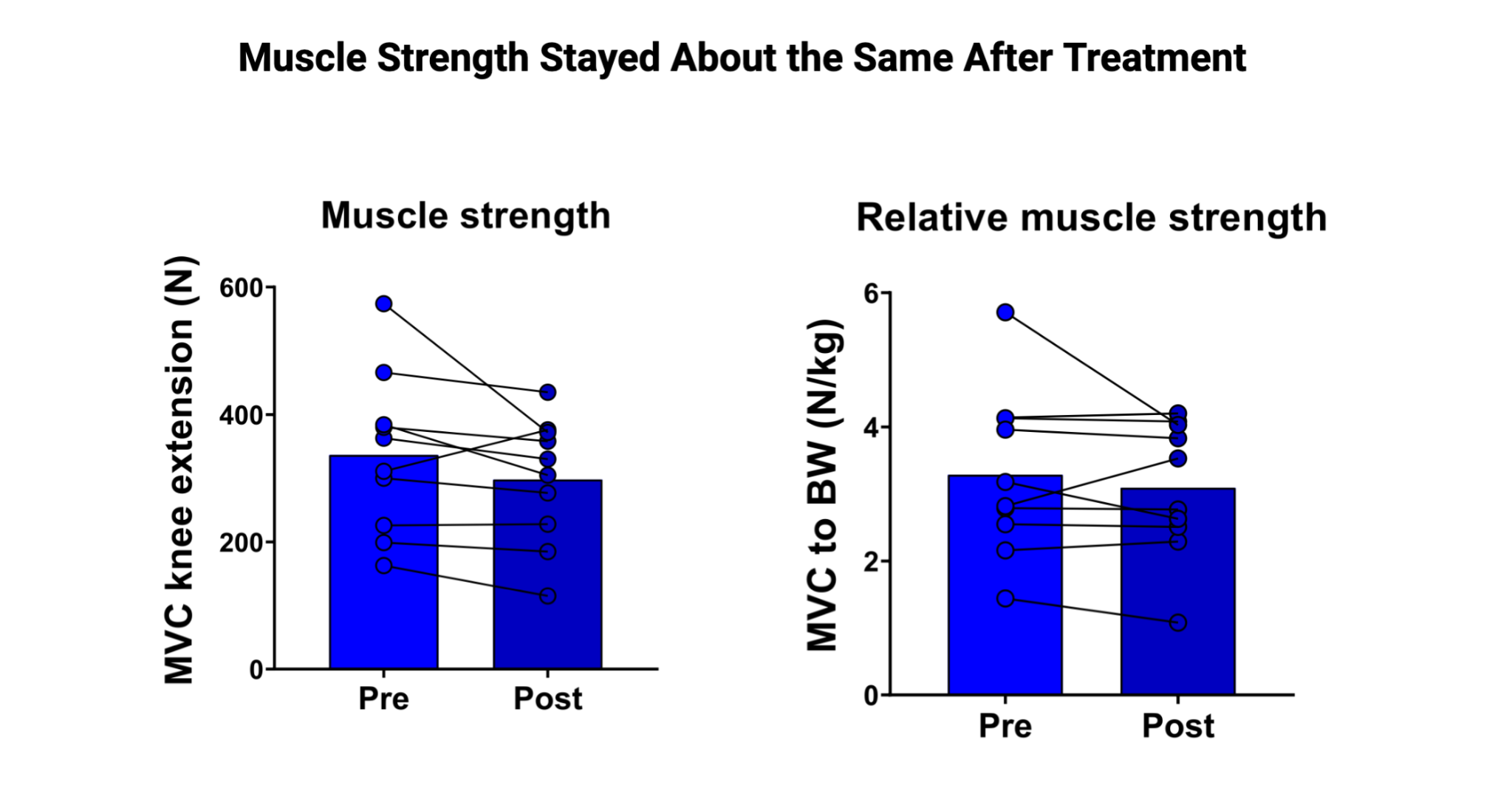
That is why muscle force generation is important. Force generation refers to the ability of muscle tissue to produce force.
In the more recent study [777], relative force generation was similar between the peptide and control conditions. Other data showed reductions in absolute force, similar to those seen with absolute muscle mass, but those reductions were not worsened by the peptide when accounting for overall body weight changes.
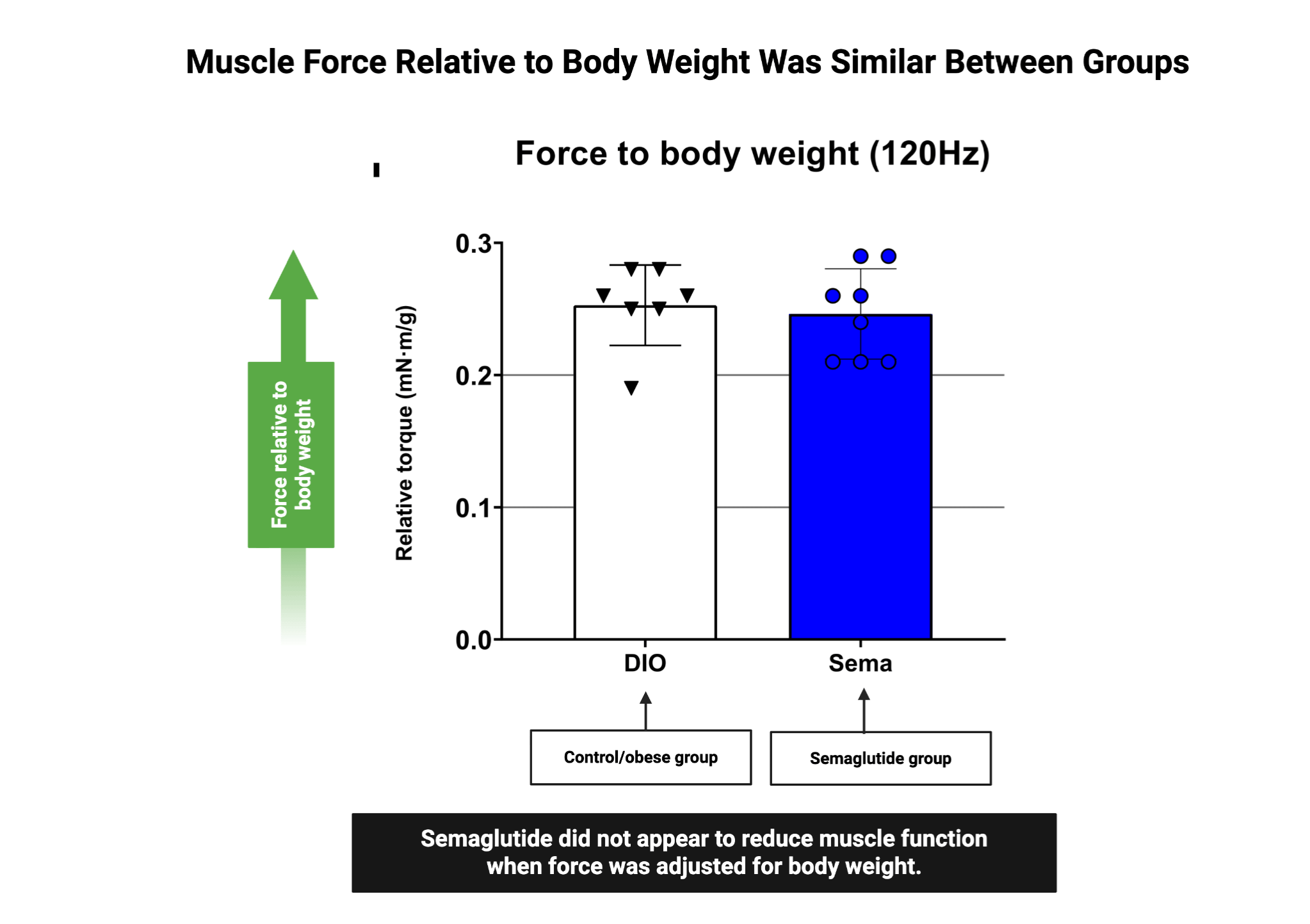
The key point is that muscle function does not appear to be uniquely harmed by peptide use. In absolute terms, there may be reductions in muscle mass and force generation, but in relative terms, both are maintained or improved.
Are Peptides Worse Than Calorie Restriction?
Another common question is whether peptides have a special muscle-loss effect that is independent of calorie restriction.
The answer leans heavily toward no.
Both calorie restriction and peptide use appear to lead to similar amounts of lean mass loss and muscle loss, assuming no exercise is added.
Early Human Evidence with Semaglutide
Moving from animal research to human evidence, the same study also included a 12-week clinical trial using semaglutide.
This was a before-and-after study, so there was no control group for comparison. That means it provides only initial human evidence and needs further confirmation.
Still, the pattern was similar. Absolute muscle mass decreased, but relative muscle mass told a different story.
The function was also not clearly defined. In fact, even absolute strength was not reduced, although that could be related to the small sample size and limited ability to detect smaller differences.
Weight loss can lead to reductions in muscle mass and muscle function, but the evidence suggests there is a disproportionate loss of fat and only a smaller loss of muscle.
More importantly, this muscle loss does not appear to be unique to peptide use. When compared with calorie restriction and other weight-loss methods, peptides do not seem to cause a uniquely harmful lean mass loss pattern.
In relative terms, muscle mass and function may be maintained or even improved when bodyweight changes are properly considered.
Pairing this with resistance training would probably heavily favor the preservation of muscle mass and function.
Main Points
Weight-loss peptides can lead to lean mass loss, and muscle is a major part of lean mass. Direct muscle weighing in animal research also shows reductions in muscle mass.
However, absolute muscle loss does not tell the full story. When muscle mass is measured relative to total bodyweight, the peptide condition does not show a disproportionate loss of muscle. This suggests the muscle-loss concern may be overstated when the data are interpreted only through absolute values.
Muscle function also appears to follow a similar pattern. Absolute force may decline, but relative force generation is not especially worsened by peptide use after accounting for bodyweight changes.
Peptides do not appear to cause a special muscle-loss effect that is clearly separate from calorie restriction. Both calorie restriction and peptide use lead to similar lean mass and muscle mass losses when exercise is not added.
Early human evidence with semaglutide shows the same general pattern: absolute muscle mass may decrease, but relative muscle mass and function do not appear to be meaningfully worsened.
Overall, weight loss can reduce muscle mass and function, but peptides appear to mostly drive fat loss, with smaller muscle-related losses that are not unique to peptide use. Pairing weight loss with resistance training would likely make muscle preservation even more favorable.
Peptides versus Dieting: Greater Risk of Lean Mass Loss?
An Odd Muscle Weakening and Rebounding Effect
Peptides on Muscle Mitochondria
Are Older People more likely to lose Lean Mass?
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
Dr. Nicolas Verhoeven, PhD / Physionic
References
[Study 777] Langer HT, Gilmore NK, Hayden CMT, et al. Weight loss with GLP-1 medicines does not result in a disproportionate loss of muscle mass or function in obese mice and humans. Cell Rep Med. 2026;7(3):102665. doi:10.1016/j.xcrm.2026.102665
Funding/Conflicts: Public Funding: From the study, support included NIH grant S10-OD025098, UC Davis T32 in Pharmacology grant T32 GM144303, National Institute of Diabetes and Digestive and Kidney Diseases grants DK139663 and DK139565, the Ministerium für Kultur und Wissenschaft des Landes Nordrhein-Westfalen, the Bundesministerium für Forschung, Technologie und Raumfahrt, German Research Foundation grants, the German Center for Diabetes Research, and the European Union; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no direct industry funding source was reported, but several conflicts were declared, including prior employment or current employment with Boehringer Ingelheim and Eli Lilly, consulting for Actimed Therapeutics, Almac Discovery, Alchemab Therapeutics, Novartis, and several food or biotech companies, co-founder roles in SinewUS and Bluewater Biotech, stock holdings in Eli Lilly and Novo Nordisk, and speaking fees from Novo Nordisk, Eli Lilly, Boehringer Ingelheim, Merck, AstraZeneca, Rhythm Pharmaceuticals, and Mercodia.
[Study 778] Linge J, Birkenfeld AL, Neeland IJ. Muscle Mass and Glucagon-Like Peptide-1 Receptor Agonists: Adaptive or Maladaptive Response to Weight Loss?. Circulation. 2024;150(16):1288-1298. doi:10.1161/CIRCULATIONAHA.124.067676
Funding/Conflicts: Public Funding: From the study, no public funding source was reported, as the listed source of funding was “None”; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, but conflicts included author relationships with AMRA Medical, Eli Lilly, BioMarin, Boehringer-Ingelheim/Lilly Alliance, Bayer, Novo Nordisk, AstraZeneca, Daiichi Sankyo, and related advisory, consulting, speaker, travel, employment, shareholder, and research-support roles.
[Study 779] Karasawa T, Choi RH, Meza CA, Rout S, Drummond MJ, Chaix A, Funai K. Unexpected effects of semaglutide on skeletal muscle mass and force-generating capacity in mice. Cell Metab. 2025;37(8):1619-1620. doi:10.1016/j.cmet.2025.07.004.
Funding/Conflicts: Public Funding: From the study, the work was supported by NIH grants DK107397, DK127979, GM144613, AG074535, CA286584, AG065993, AG076075, and AG086328, and by a Japan Society for the Promotion of Science Fellows grant-in-aid, 24KJ2039; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, and the authors declared no competing interests.
[Study 780] Look M, Dunn JP, Kushner RF, et al. Body composition changes during weight reduction with tirzepatide in the SURMOUNT-1 study of adults with obesity or overweight. Diabetes Obes Metab. 2025;27(5):2720-2729. doi:10.1111/dom.16275
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, the work was funded by Eli Lilly and Company; conflicts included speaker, lecture, advisory, or consulting relationships with Eli Lilly and Company and other companies, and several authors were employees and shareholders of Eli Lilly and Company.