
This Peptide Reverses Osteoarthritis!

Main Points
Osteoarthritis involves three major problems: pain, inflammation, and cartilage destruction. Preclinical evidence suggests liraglutide and similar peptides may reduce pain, lower inflammatory signaling, and reduce cartilage breakdown in osteoarthritis.
Semaglutide showed evidence of improving osteoarthritis outcomes in a small human clinical trial. The peptide group had greater improvement in WOMAC scores, which measure arthritis-related pain and function, compared with the control group.
The most striking finding was an increase in cartilage thickness in the peptide-treated condition. That suggests the benefit may go beyond symptom relief and may involve cartilage rejuvenation.
The key caution is that the human clinical trial was small, cartilage assessments appeared to be unblinded, and the study was not properly controlled to prove that the human benefits were independent of weight loss. Also, the evidence focused on metabolically tied osteoarthritis, so the results may not apply equally to every form of osteoarthritis.
Overall, semaglutide and related peptides show early but promising evidence for reducing osteoarthritis symptoms, protecting cartilage, and possibly supporting cartilage recovery, especially in overweight individuals or metabolically related osteoarthritis.
Peptides are getting a lot of attention right now, often for fat loss and metabolic health, but their potential benefits may extend beyond metabolism. Emerging evidence suggests that certain peptides may reduce osteoarthritis symptoms and may even help restore cartilage in humans.
Osteoarthritis can be understood through three major problems: pain, inflammation, and cartilage destruction. These are the three major “horsemen” that make the condition painful, limiting, and progressive.
The First Problem: Pain
In preclinical studies [730], researchers tested the impact of liraglutide, a peptide in the same general class as semaglutide, on osteoarthritis-related pain.
The goal was to see whether the animals had a higher pain threshold. In this type of testing, a higher threshold means more pressure or stimulation is needed before pain is experienced. Higher doses of liraglutide improved pain-related outcomes in osteoarthritic animals.
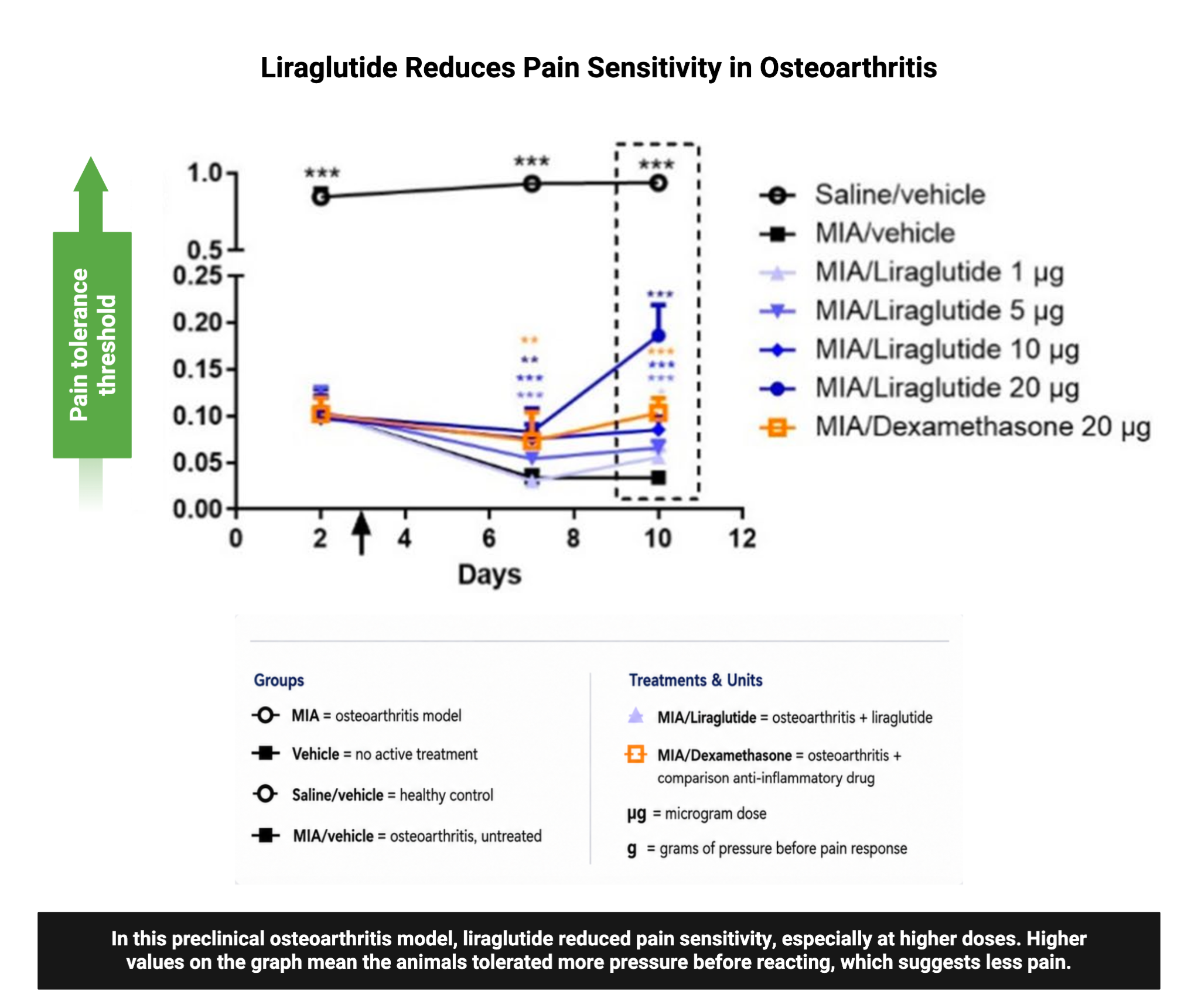
So, the first major finding is that liraglutide and similar peptides reduced pain in preclinical osteoarthritis data.
The Second Problem: Inflammation
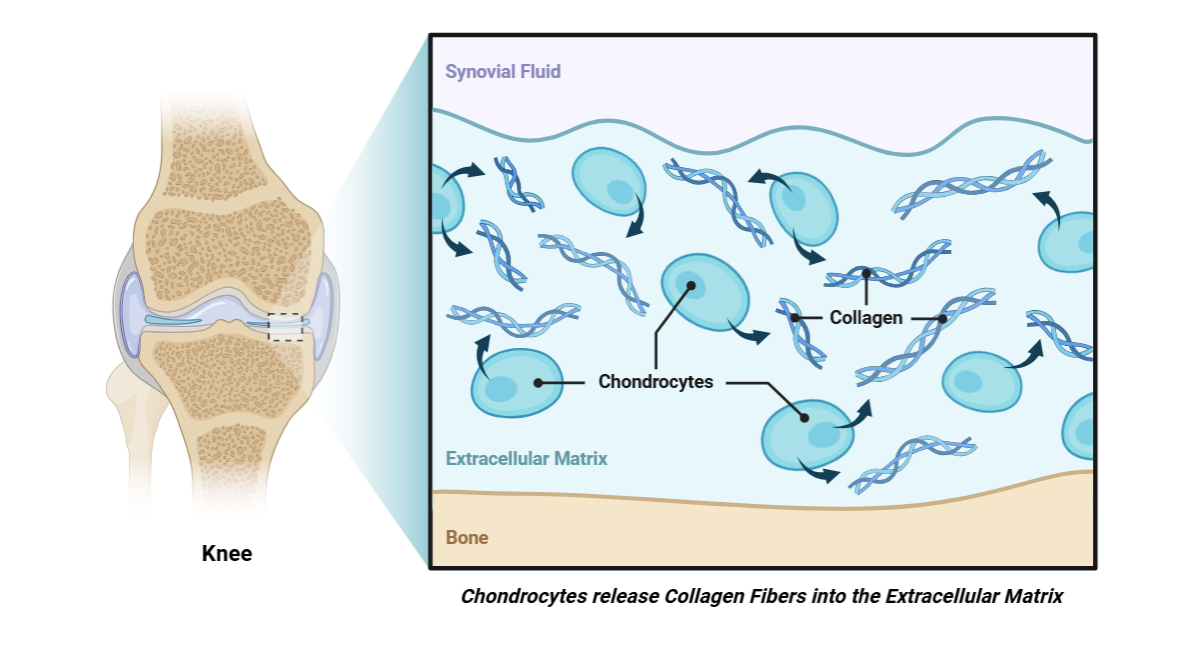
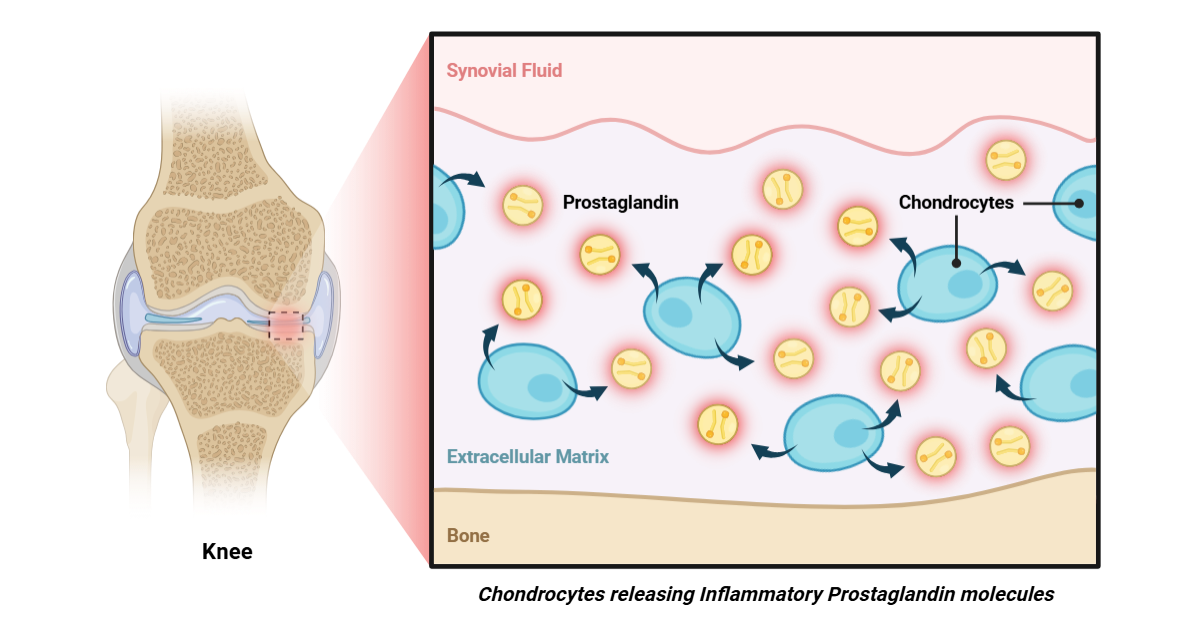
The next issue is inflammation. To understand this, we need to look at chondrocytes, which are cells found in the joints. Chondrocytes help release collagen and other structural proteins that maintain joint structure.
But they can also release inflammatory molecules that attract immune cells into the joint area.
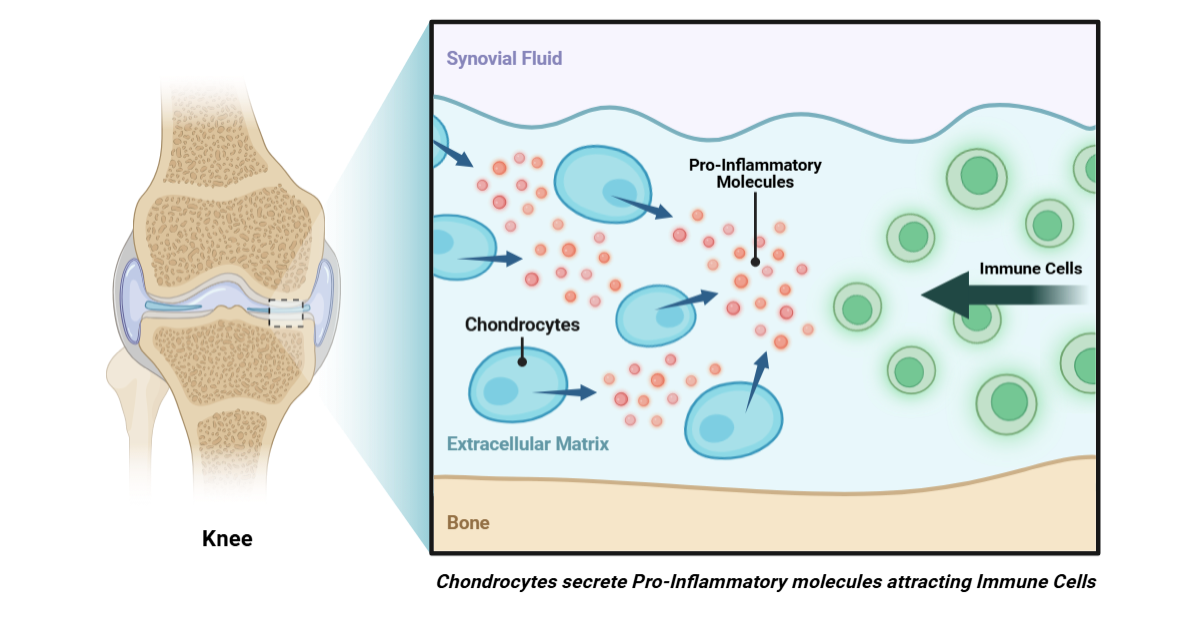
In osteoarthritis, inflammation increases. That can lead to more immune cell invasion and more joint damage. Researchers measured inflammatory molecules produced by joint-associated chondrocytes.
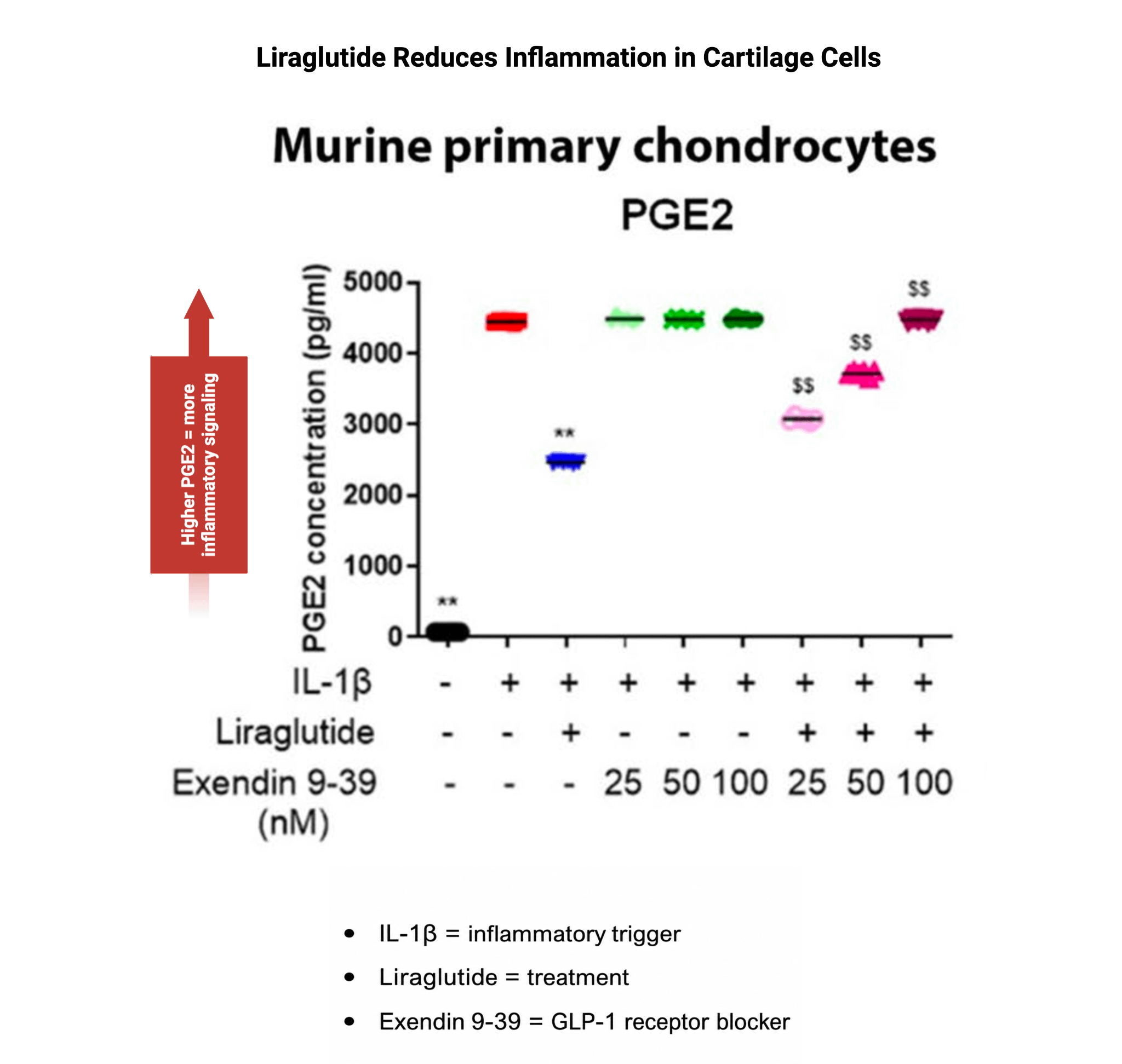
One important molecule was PGE, or prostaglandin. Prostaglandins are fat-derived molecules that can contribute to swelling, pain sensitivity, and more inflammation. In this context, lower PGE is better.
When an inflammatory molecule was added, PGE rose sharply. But when liraglutide was added alongside that inflammatory trigger, PGE levels dropped by about half. That suggests liraglutide reduced inflammatory signaling in these joint cells.
So, the second major finding is that inflammation was reduced by liraglutide and similar peptides in preclinical osteoarthritis studies.
The Third Problem: Cartilage Destruction
The final problem is cartilage destruction.
In the same study, researchers measured structural loss in the joint. The joint’s architecture includes molecules called glycosaminoglycans, which help form and support cartilage structure. When these molecules are cut or broken away from cartilage, that indicates the cartilage architecture is being destroyed.
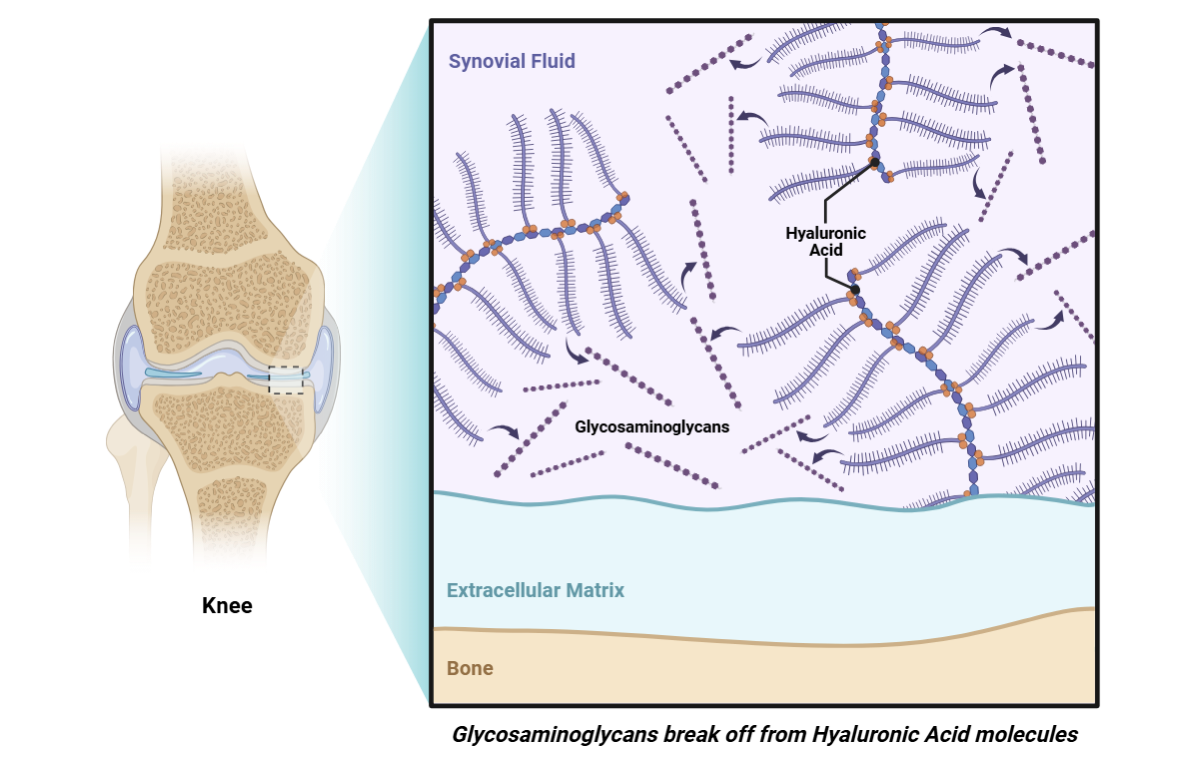
In the peptide-treated conditions, there was less release of glycosaminoglycans. That suggests less cartilage structure was being broken down.
Peptide’s Mechanisms for Osteoarthritis Benefit
More on Peptide’s Weight Loss Independent Effects
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
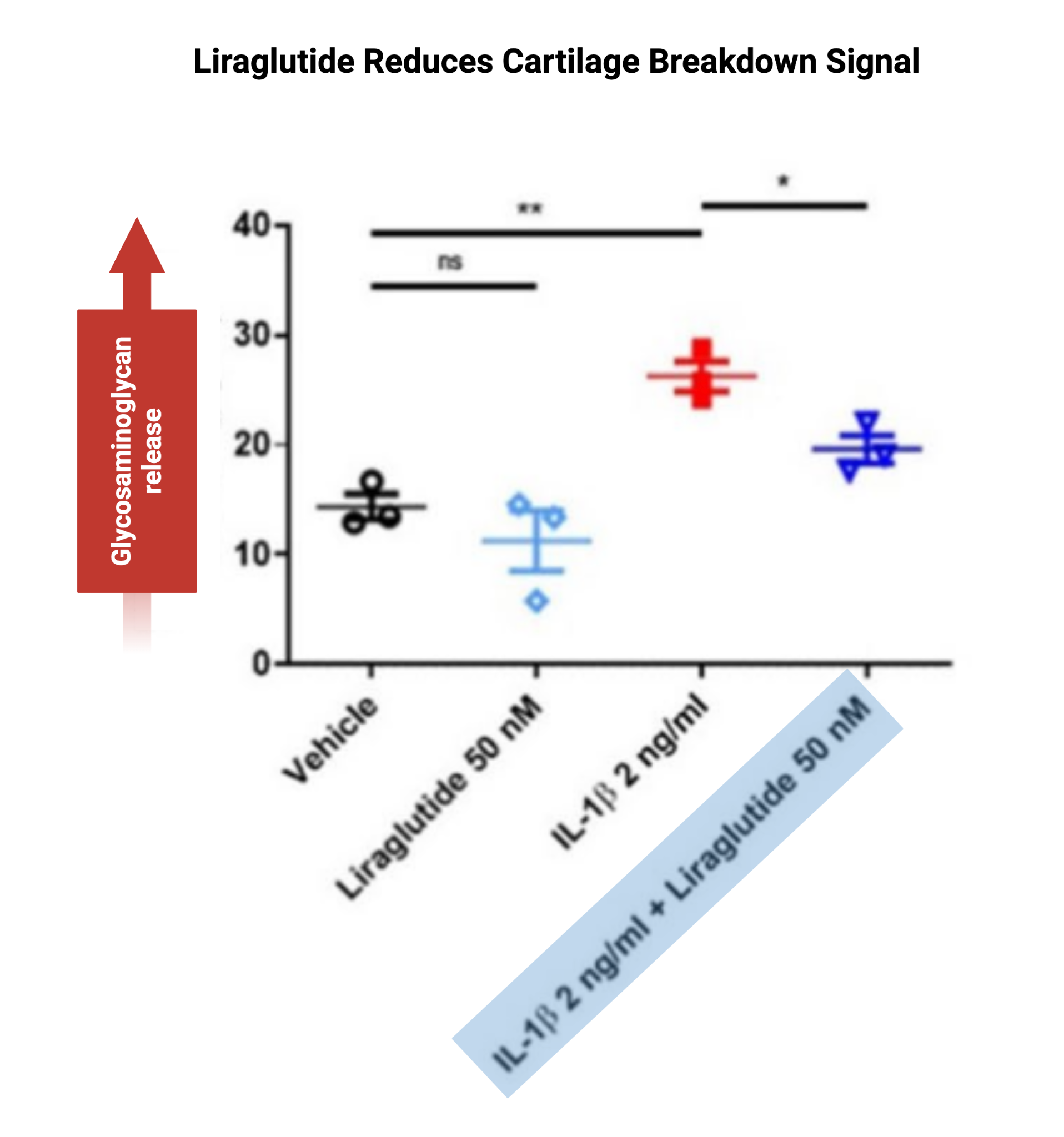
So, the third major finding is that cartilage destruction was also reduced with liraglutide in preclinical evidence.
Evidence of Cartilage Preservation and Possible Renewal
Another study [729] showed images of cartilage showing that osteoarthritis meaningfully reduced cartilage.The osteoarthritic condition showed cartilage loss, as expected. But when the peptide was included, more cartilage appeared to be present.
That suggests preservation and possibly renewal of cartilage.
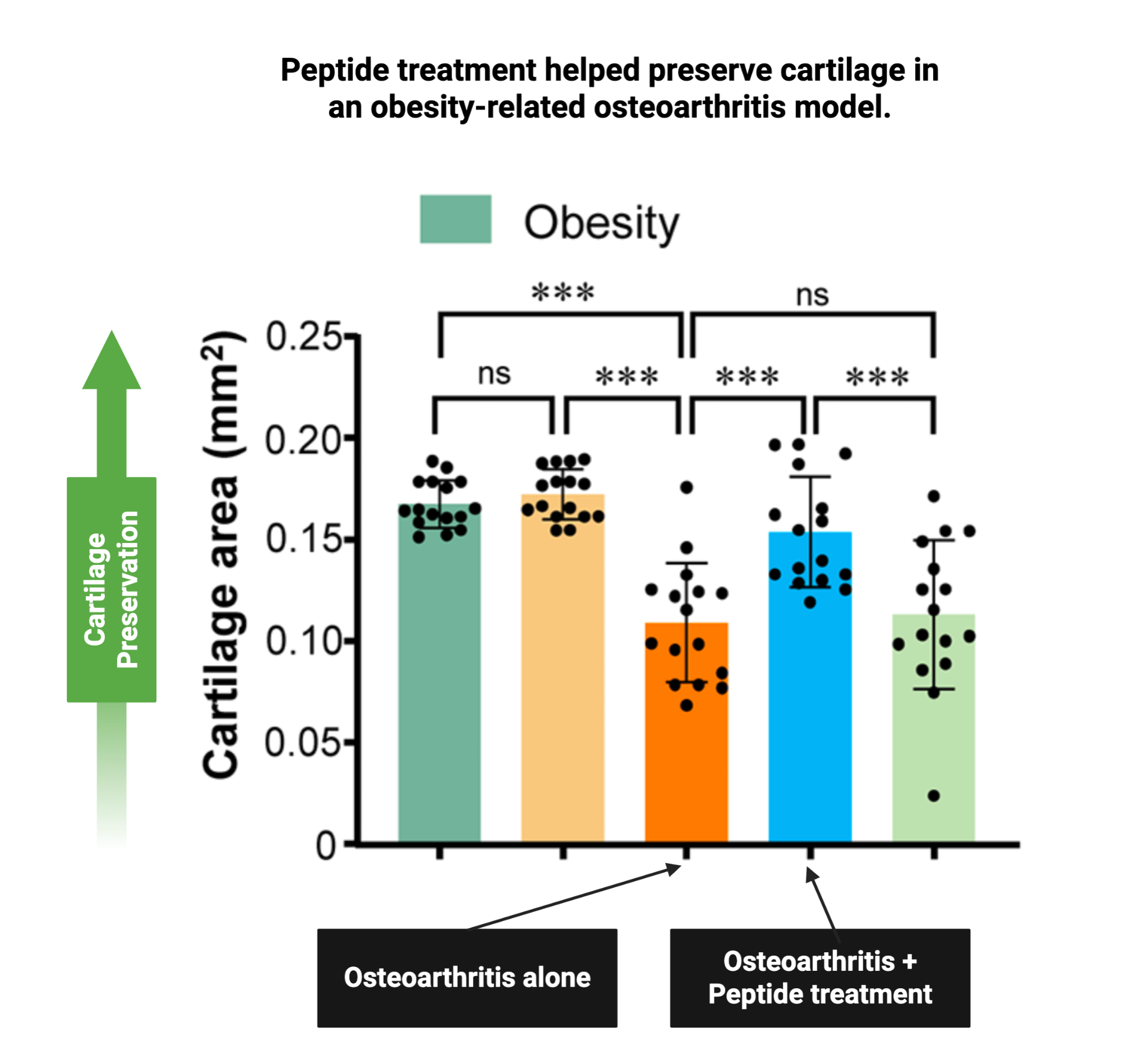
This was also supported by averaged data (figure seen above). The osteoarthritis-only condition showed worse cartilage outcomes, while the peptide-treated condition showed better cartilage preservation.
Human Evidence: A Small Clinical Trial
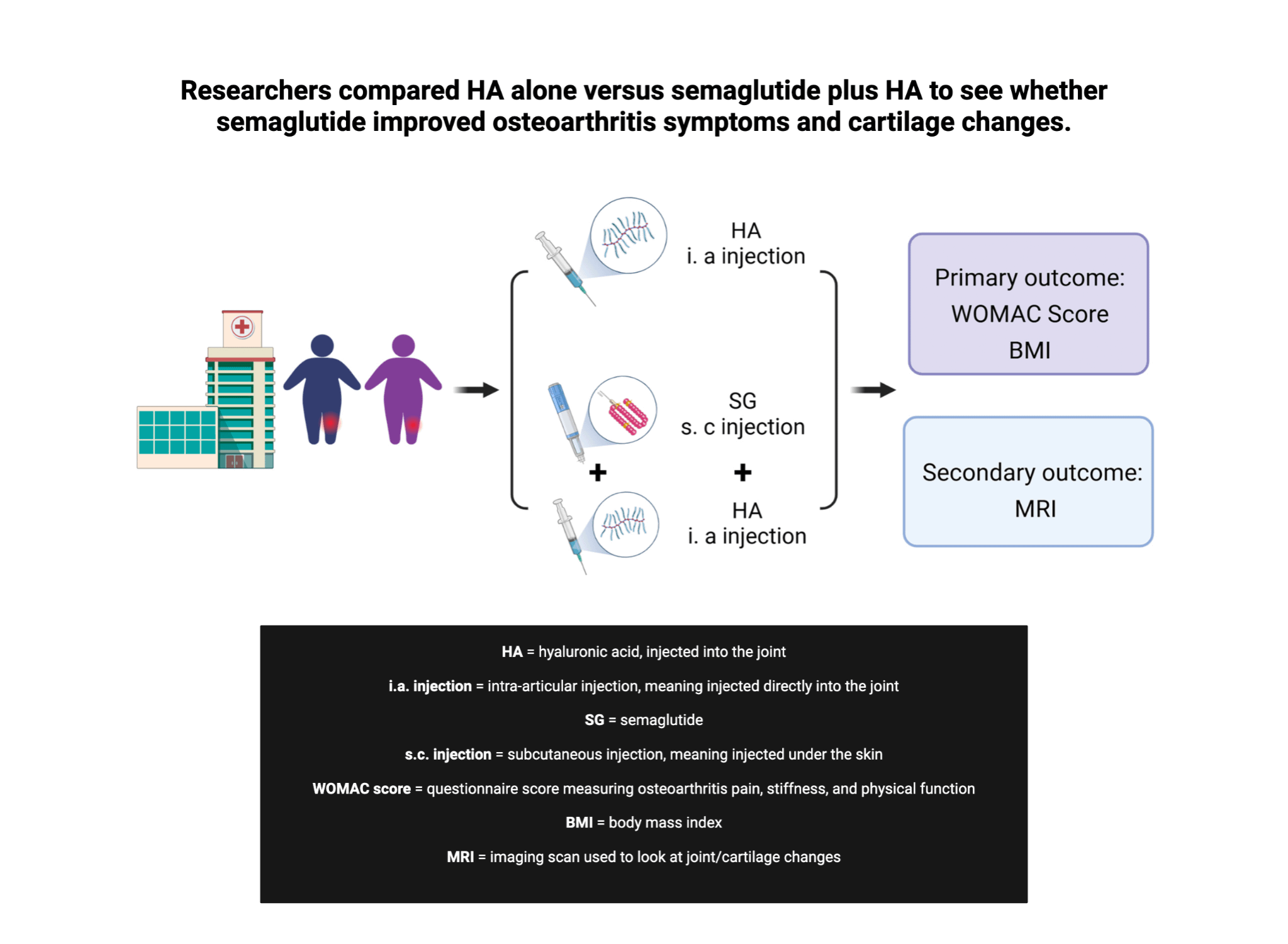
The most important part is that this did not stop at animal or cell data. Researchers also conducted a small clinical trial in humans.
In the study design, the control group received an injection of hyaluronic acid. The peptide group received the peptide along with the same injection of hyaluronic acid. The main outcome was the WOMAC score, which measures arthritis-related pain and function.
After 24 weeks, both groups appeared to improve, suggesting hyaluronic acid may have had some benefit. But the greater benefit occurred in the peptide co-administration group.
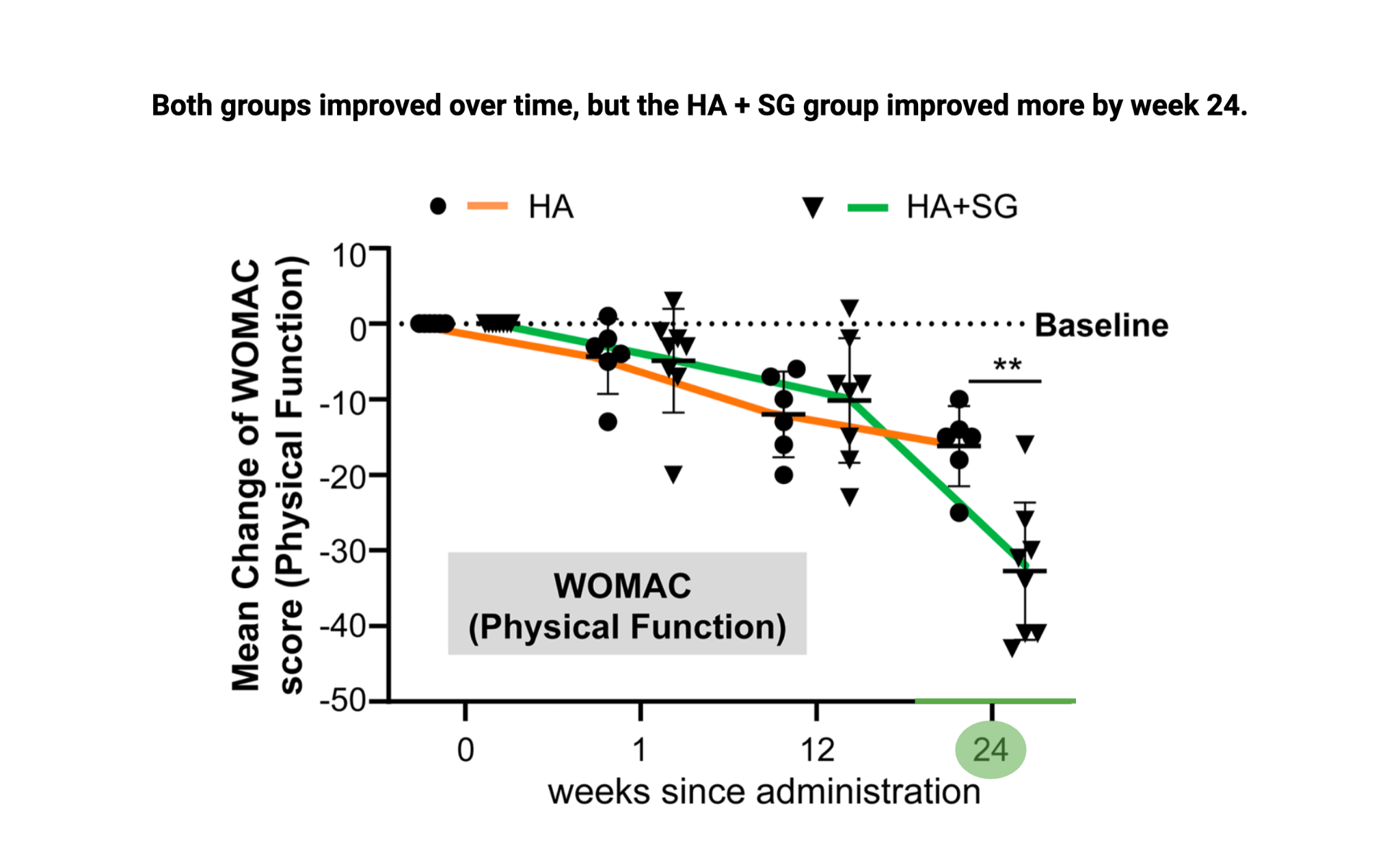
That suggests the peptide improved osteoarthritis symptoms in this small study.
Cartilage Thickness Increased
The researchers also measured cartilage thickness. This is especially important because the data showed an increase in cartilage in the peptide-treated condition.
An increase matters because it suggests more than symptom relief. It suggests cartilage rejuvenation.
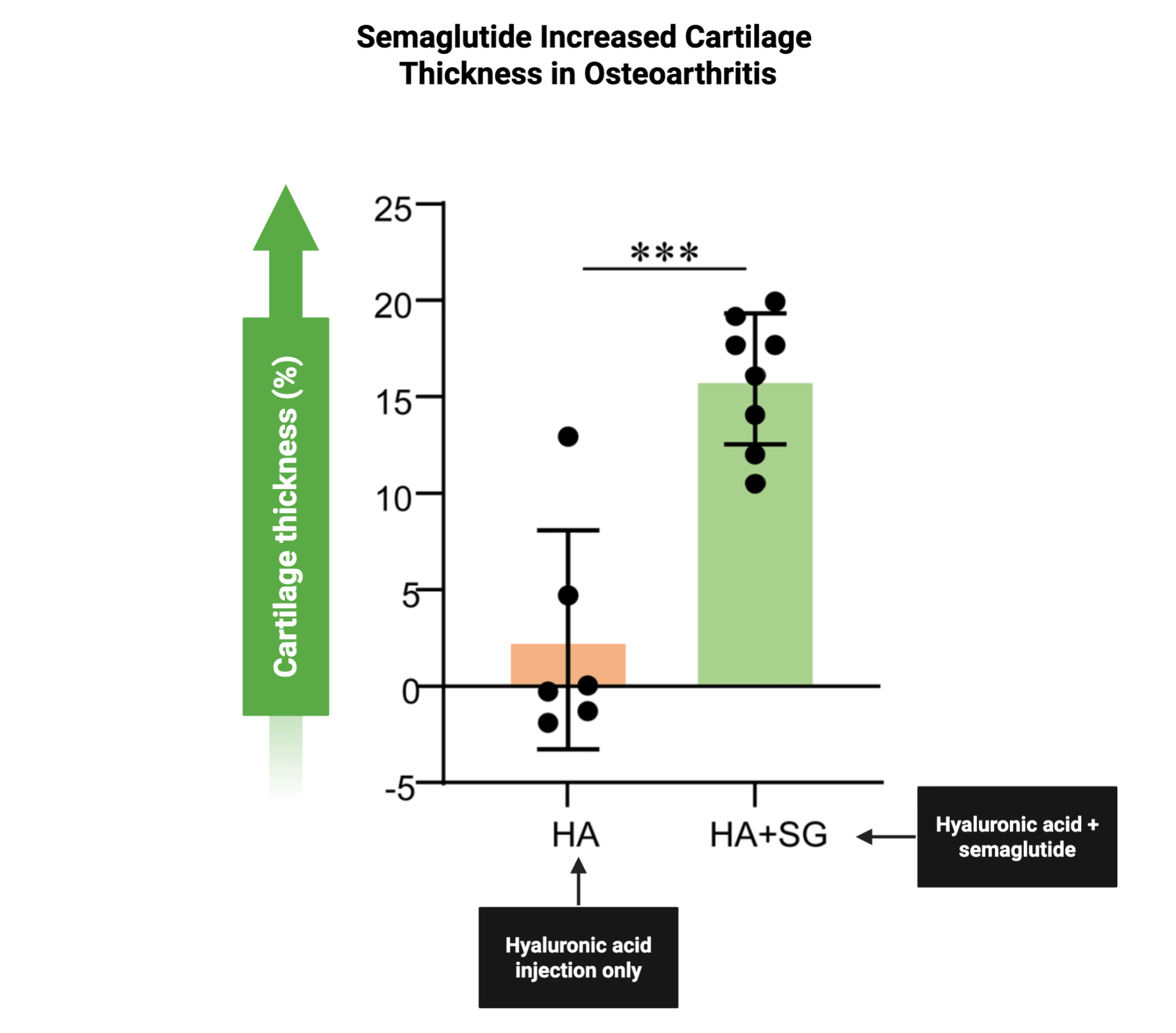
These data indicate that the peptide reduced osteoarthritis symptoms, improved life with osteoarthritis, and rejuvenated cartilage affected by osteoarthritis in a small clinical trial.
That peptide was semaglutide [729], and it belongs to the same general family as liraglutide.
There are important limitations to consider, however
First, as far as the evidence indicates, the animal and human cartilage assessments appeared to be unblinded. That means the assessors may have known which condition the data belonged to. This can introduce bias.
Second, the study [729] claimed that semaglutide produced osteoarthritis benefits independent of weight loss. That would be a major finding because weight loss itself can reduce stress on osteoarthritic joints. However, the human data were not properly controlled to prove whether the effect was truly independent of weight loss.
Third, the clinical study was small. That does not erase the results, but it should make us cautious about overstating them.
Even with those limitations, the findings are exciting because long-term associative studies [731] also support the possibility that these peptides may benefit osteoarthritis. Those studies are not clinical trials, so they cannot prove cause and effect in the same way. But they do support the mechanistic and early clinical evidence, including the possibility that some benefits may be independent of weight loss.
What the Larger Associative Evidence Suggests
The evidence is still early. But there is enough to suggest that semaglutide and similar peptides lean toward having an osteoarthritis benefit, at least in overweight individuals.
That benefit may extend beyond symptom relief and may involve some recovery from osteoarthritis-related cartilage damage. Some of the effects may also be independent of weight loss.
However, the study [729] focused on a metabolic cause of osteoarthritis. That means the effects may not be the same across all types or causes of osteoarthritis.
More research is still needed.
Main Points
Osteoarthritis involves three major problems: pain, inflammation, and cartilage destruction. Preclinical evidence suggests liraglutide and similar peptides may reduce pain, lower inflammatory signaling, and reduce cartilage breakdown in osteoarthritis.
Semaglutide showed evidence of improving osteoarthritis outcomes in a small human clinical trial. The peptide group had greater improvement in WOMAC scores, which measure arthritis-related pain and function, compared with the control group.
The most striking finding was an increase in cartilage thickness in the peptide-treated condition. That suggests the benefit may go beyond symptom relief and may involve cartilage rejuvenation.
The key caution is that the human clinical trial was small, cartilage assessments appeared to be unblinded, and the study was not properly controlled to prove that the human benefits were independent of weight loss. Also, the evidence focused on metabolically tied osteoarthritis, so the results may not apply equally to every form of osteoarthritis.
Overall, semaglutide and related peptides show early but promising evidence for reducing osteoarthritis symptoms, protecting cartilage, and possibly supporting cartilage recovery, especially in overweight individuals or metabolically related osteoarthritis.
Peptide’s Mechanisms for Osteoarthritis Benefit
More on Peptide’s Weight Loss Independent Effects
All of these topics are explored in depth in the complete analysis, along with access to a private podcast, live sessions, a growing research library, and practical breakdowns—available exclusively to Physionic Insiders.
Dr. Nicolas Verhoeven, PhD / Physionic
References
[Study 729] Qin H, Yu J, Yu H, et al. Semaglutide ameliorates osteoarthritis progression through a weight loss-independent metabolic restoration mechanism. Cell Metab. 2026;38:582-597. doi:10.1016/j.cmet.2026.01.008
Funding/Conflicts: Public Funding: From the study, the project was supported by National Natural Science Foundation of China grants, Shenzhen Medical Research Funds, and Shenzhen Science and Technology Research Funding; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, and the authors declared no competing interests.
[Study 730] Meurot C, Martin C, Sudre L, et al. Liraglutide, a glucagon-like peptide 1 receptor agonist, exerts analgesic, anti-inflammatory and anti-degradative actions in osteoarthritis. Sci Rep. 2022;12:1567. doi:10.1038/s41598-022-05323-7
Funding/Conflicts: Public Funding: From the study, no public funding source was reported; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no direct industry funding source was reported, but several authors were affiliated with 4P-Pharma and/or 4Moving Biotech, and conflicts included personal fees from multiple pharmaceutical companies, a TRB Chemedica grant, leadership roles in 4Moving Biotech and 4P Pharma, and patents owned by 4Moving Biotech and Sorbonne University for the use of GLP-1 analogs in osteoarthritis.
[Study 731] Zhu H, Zhou L, Wang Q, et al. Glucagon-like peptide-1 receptor agonists as a disease-modifying therapy for knee osteoarthritis mediated by weight loss: findings from the Shanghai Osteoarthritis Cohort. Ann Rheum Dis. 2023;82:1218-1226. doi:10.1136/ard-2023-223845
Funding/Conflicts: Public Funding: From the study, the work was funded by the Shanghai Shen Kang Hospital Development Centre, Clinical Research Plan of SHDC, and the National Natural Science Foundation of China; Non-Profit Funding: From the study, no non-profit funding source was reported; Industry Funding: From the study, no industry funding source was reported, and the authors declared no competing interests.